
1/ In the🥉@PaChapterACC & @CardioNerds Narratives in Cardiology episode @mirmerrill, @scfuentesr, and @NatashaCuk talk w/ @KTamirisaMD
Follow this #CardsNarratives🧵on the discussion about gender equity & women in Cardiology/Electrophysiology (EP)
Follow this #CardsNarratives🧵on the discussion about gender equity & women in Cardiology/Electrophysiology (EP)

2/ We'll cover these 3 questions:
🔸Why should we promote gender diversity in Cardiology/EP?
🔸How do we address barriers for women in Cardiology/EP?
🔸What are some opportunities for EP in private practice?
🔸Why should we promote gender diversity in Cardiology/EP?
🔸How do we address barriers for women in Cardiology/EP?
🔸What are some opportunities for EP in private practice?
3/ I feel comfortable openly discussing or asking others about factors that make them different from myself like race, religion, ethnicity, gender, sexual orientation, immigration status, etc
4/ Women are🦄in procedural subspecialties of cardiology
Women only 7-10% of EPs in practice & limited visibility in leadership roles
Why is diversity important❓
♦️ Diversity drives innovation
♦️ Women more likely to provide patient centered communication➡️improve outcomes
Women only 7-10% of EPs in practice & limited visibility in leadership roles
Why is diversity important❓
♦️ Diversity drives innovation
♦️ Women more likely to provide patient centered communication➡️improve outcomes

5/ Addressing barriers to EP:
🔹⬆️Inclusivity by adjusting work & training environments
🔹Address sexual harassment & discrimination
🔹Advocate for work-life integration & flexible work schedules
🔹Acknowledge & respond to family planning concerns
bit.ly/3syVECS
🔹⬆️Inclusivity by adjusting work & training environments
🔹Address sexual harassment & discrimination
🔹Advocate for work-life integration & flexible work schedules
🔹Acknowledge & respond to family planning concerns
bit.ly/3syVECS

6/ ACC survey of hostility, discrimination, harassment in cardiology workplace by @DrLaxmiMehta ⤵️
jacc.org/doi/abs/10.101…
jacc.org/doi/abs/10.101…

7/ Other ways to address barriers of women in Cardiology/EP:
♦️ Consider reduced or flexible training schedules
♦️ Address underrepresentation in leadership
♦️ Address the unequal access to funding & resources, pay & compensation inequity
jacc.org/doi/10.1016/j.…
♦️ Consider reduced or flexible training schedules
♦️ Address underrepresentation in leadership
♦️ Address the unequal access to funding & resources, pay & compensation inequity
jacc.org/doi/10.1016/j.…

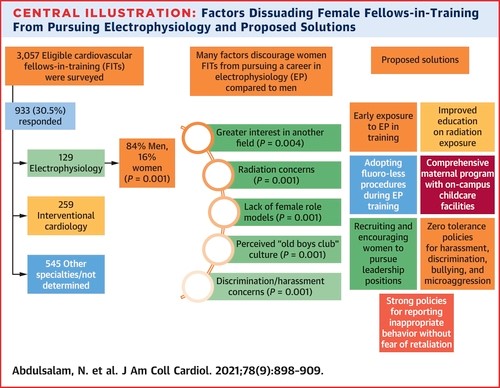
8/ Sex differences in pursuit of IC as subspecialty among FITs: jacc.org/doi/full/10.10…
🛑Similar barriers apply to EP🛑
Graph depicting barriers ⤵️
🛑Similar barriers apply to EP🛑
Graph depicting barriers ⤵️

9/ Survey of FITs⤵️
14% FITs interested in EP
Among those interested, only 16% women
Women more likely to pursue career in EP if they had female mentor
Article: jacc.org/doi/10.1016/j.…
Editorial: jacc.org/doi/10.1016/j.…
14% FITs interested in EP
Among those interested, only 16% women
Women more likely to pursue career in EP if they had female mentor
Article: jacc.org/doi/10.1016/j.…
Editorial: jacc.org/doi/10.1016/j.…
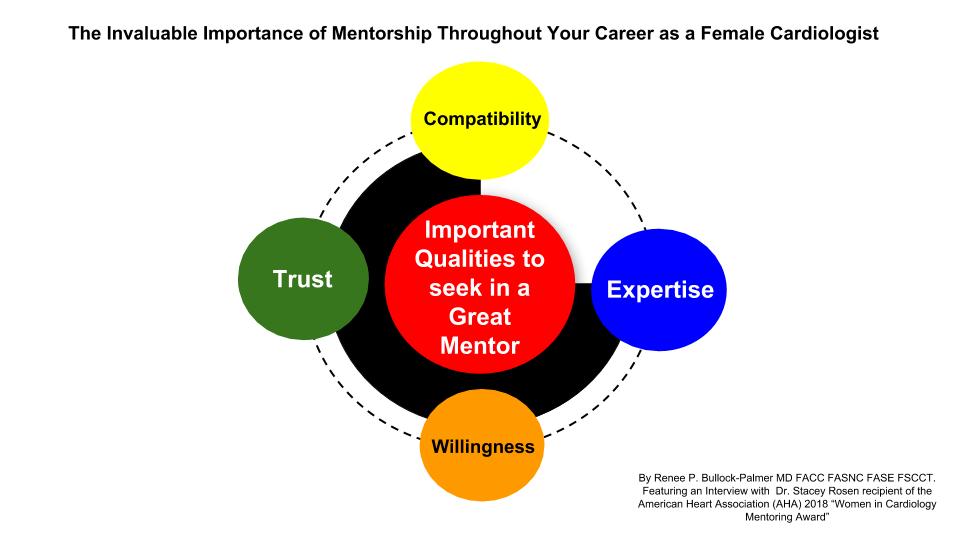
10/ Mentorship from women & men is 🔑
✨Good listener
✨Empower mentees
✨Provide constructive criticism/feedback
✨Be honest, show vulnerability/imperfections
Role models also important – see what someone went through, learn from their journey
Figure by @RBP0612
✨Good listener
✨Empower mentees
✨Provide constructive criticism/feedback
✨Be honest, show vulnerability/imperfections
Role models also important – see what someone went through, learn from their journey
Figure by @RBP0612
11/ Other practical tips for Women in Cardiology/EP
💠Women have⬇️speaking invitations: step up & say I am interested
💠Put interests out there, be your own advocate
💠Sponsorship: asked to write paper/ give talk but don't have time➡️invite colleague
pubmed.ncbi.nlm.nih.gov/33587663/
💠Women have⬇️speaking invitations: step up & say I am interested
💠Put interests out there, be your own advocate
💠Sponsorship: asked to write paper/ give talk but don't have time➡️invite colleague
pubmed.ncbi.nlm.nih.gov/33587663/

12/ Addressing bias
🛑Microaggressions: pick your battles
🛑Negative encounter in workplace: have conversation, ask them "did you really mean it?"
🛑Repetitive & intentional: call it out, use allies
Silence communicates approval, so speak up
amjmed.com/article/S0002-…
🛑Microaggressions: pick your battles
🛑Negative encounter in workplace: have conversation, ask them "did you really mean it?"
🛑Repetitive & intentional: call it out, use allies
Silence communicates approval, so speak up
amjmed.com/article/S0002-…

13/ Addressing imposter syndrome
Everyone doubts their abilities, but not all talk about it
Plural view helps – you are not the only one
➕Positive feedback for yourself- think about great things you've done
✍️Journal positives & negatives
bit.ly/37ZHpxl
Everyone doubts their abilities, but not all talk about it
Plural view helps – you are not the only one
➕Positive feedback for yourself- think about great things you've done
✍️Journal positives & negatives
bit.ly/37ZHpxl
14/ Benefits of EP private practice
💮Certain level of independence and flexibility, can choose devices/tools, lab set-up, build new program
💮Leadership opportunities, can be part of decision-making
💮Close & longitudinal relationships w/ patients
💮Certain level of independence and flexibility, can choose devices/tools, lab set-up, build new program
💮Leadership opportunities, can be part of decision-making
💮Close & longitudinal relationships w/ patients
15/ More on EP private practice:
💮Can engage w/ community initiatives in addition to procedures, patient care, & leadership opportunities
☠️Understanding finances is important – take time to learn about this from mentors
☠️May be harder to network when outside of academia
💮Can engage w/ community initiatives in addition to procedures, patient care, & leadership opportunities
☠️Understanding finances is important – take time to learn about this from mentors
☠️May be harder to network when outside of academia
16/ Summary
🔹Women are underrepresented in EP
🔹Need to mentor & address barriers (culture, work conditions, underrepresentation in leadership)
🔹Private practice EP involves procedures, patient care, leadership, & community engagement opportunities
go.nature.com/3mnhecC
🔹Women are underrepresented in EP
🔹Need to mentor & address barriers (culture, work conditions, underrepresentation in leadership)
🔹Private practice EP involves procedures, patient care, leadership, & community engagement opportunities
go.nature.com/3mnhecC

17/ I feel comfortable openly discussing or asking others about factors that make them different from myself like race, religion, ethnicity, gender, sexual orientation, immigration status, etc
18/ After reading this #CardsNarratives Tweetorial, I have a greater appreciation for diversity in cardiology.
19/ Please consider replying with a personal experience or reflection in relation to anything discussed in this Tweetorial
20/ Listen to the full discussion here w/ Dr. Tamirisa on "Empowerment and Growing Together as Women in EP"
cardionerds.com/141-narratives…
Thanks to @CardioNerds, @AmitGoyalMD, @Dr_DanMD, @ThomasMDas for guidance and feedback on this #CardsNarratives Tweetorial!
cardionerds.com/141-narratives…
Thanks to @CardioNerds, @AmitGoyalMD, @Dr_DanMD, @ThomasMDas for guidance and feedback on this #CardsNarratives Tweetorial!

• • •
Missing some Tweet in this thread? You can try to
force a refresh




















