Dear FDA Advisory Ctte:
As you consider boosters for older Americans, ask yourselves *why*.
Is it to:
1. Slow transmission,
2. Boost long-term (waning?) immunity, or
3. Give short-term protection?
1. Will be a small effect
2. Has no data
3. May be the wrong time.
A thread...
As you consider boosters for older Americans, ask yourselves *why*.
Is it to:
1. Slow transmission,
2. Boost long-term (waning?) immunity, or
3. Give short-term protection?
1. Will be a small effect
2. Has no data
3. May be the wrong time.
A thread...
1a. For transmission, look at the data from Israel. After giving booster shots, rates in those 60+ went down sharply.
But what was the effect on other groups? None.
ourworldindata.org/vaccination-is…
But what was the effect on other groups? None.
ourworldindata.org/vaccination-is…

1b. This makes sense, because:
(a) in the US, people 65+ have the lowest case rates
(b) most of those cases are in not-fully-vax'd
(c) fully vax'd recover faster
(d) people 65+ have fewer contacts
Bottom line: to halt transmission, fully vax'd seniors would be lowest priority.
(a) in the US, people 65+ have the lowest case rates
(b) most of those cases are in not-fully-vax'd
(c) fully vax'd recover faster
(d) people 65+ have fewer contacts
Bottom line: to halt transmission, fully vax'd seniors would be lowest priority.

2a. Earliest data on immunity come from those fully vax'd by Jan 31 (bit.ly/2VBogPX).
We have almost no data at 8 months, no data on long-term booster effectiveness.
If is to bolster long-term immunity, recommending boosters w/o data seriously harms FDA credibility.
We have almost no data at 8 months, no data on long-term booster effectiveness.
If is to bolster long-term immunity, recommending boosters w/o data seriously harms FDA credibility.
2b. Side notes on the data from Israel:
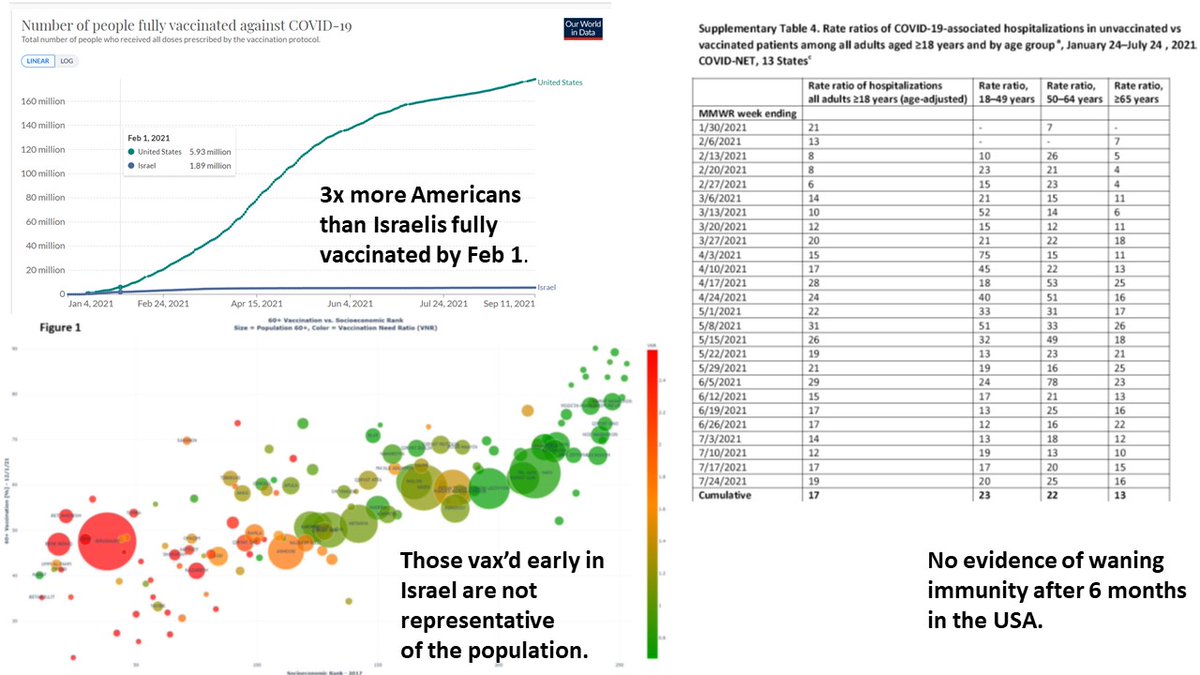
a) USA had 3x more people vax'd by Feb 1.
b) Early vax'ers in Israel are not representative of the population (bit.ly/390Rcnr).
c) No evidence of waning immunity in the USA (bit.ly/3lgLV0S).
Why not trust larger US data?
a) USA had 3x more people vax'd by Feb 1.
b) Early vax'ers in Israel are not representative of the population (bit.ly/390Rcnr).
c) No evidence of waning immunity in the USA (bit.ly/3lgLV0S).
Why not trust larger US data?
2c. Data cited for waning immunity (bit.ly/3kba6P7):
a) are 6 months post-vax
b) have strong confounders (lower rates if Arab/Jan vax than Jewish/May vax)
c) ignore larger datasets (bit.ly/3Ele7sj, bit.ly/3lgLV0S), also 6 months post-vax, w/o waning
a) are 6 months post-vax
b) have strong confounders (lower rates if Arab/Jan vax than Jewish/May vax)
c) ignore larger datasets (bit.ly/3Ele7sj, bit.ly/3lgLV0S), also 6 months post-vax, w/o waning

2d. To summarize:
a) At 6 months, vax still working very well.
b) Data on waning are unconvincing.
c) Essentially no data at 8 months post-2nd dose.
d) Zero data on long-term effectiveness of boosters.
If goal is to bolster long-term immunity, there is no data-driven rationale.
a) At 6 months, vax still working very well.
b) Data on waning are unconvincing.
c) Essentially no data at 8 months post-2nd dose.
d) Zero data on long-term effectiveness of boosters.
If goal is to bolster long-term immunity, there is no data-driven rationale.
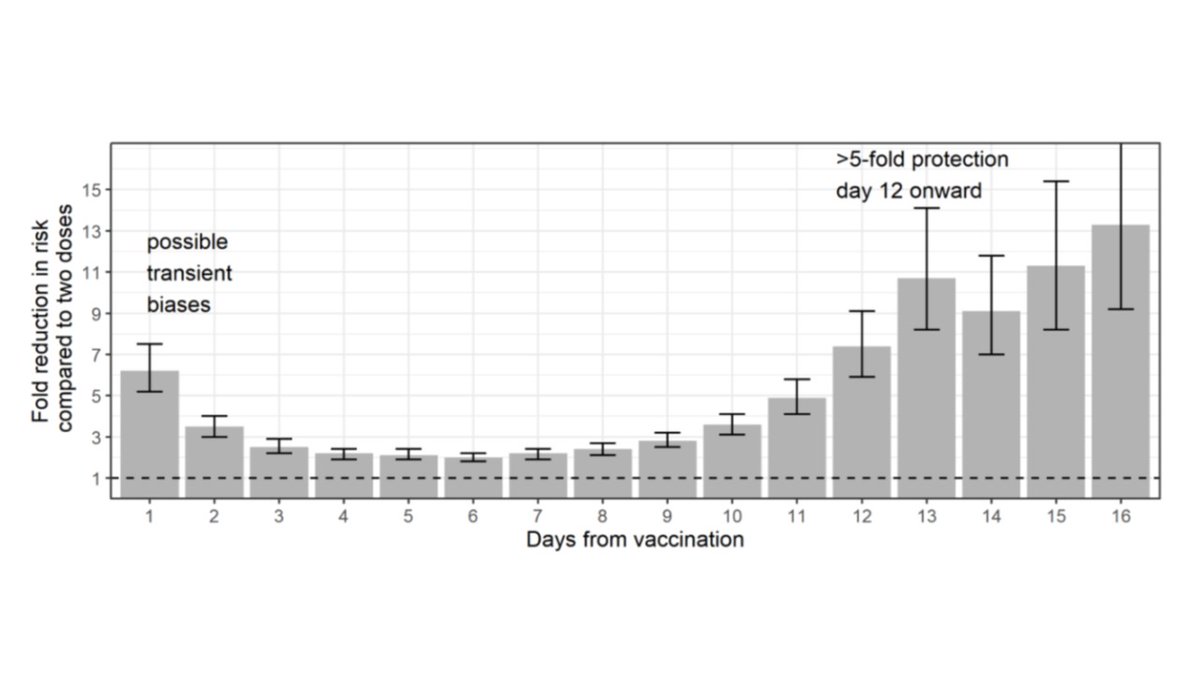
3a. What's left is a short-term protective effect of a booster shot.
This is undoubtedly a real thing.
See data above on rates after booster in Israel, also below from bit.ly/2VyUWJI.
But this shouldn't be conflated w long-term protection.
This is undoubtedly a real thing.
See data above on rates after booster in Israel, also below from bit.ly/2VyUWJI.
But this shouldn't be conflated w long-term protection.
3b. This is like comparing:
Person A who got sick in Jan and again 2 wks ago, vs
Person B who only got sick in Jan.
Person A will be protected for a while, because their immune system (mostly antibodies) is ramped up.
But 6 months from now, there might not be any difference.
Person A who got sick in Jan and again 2 wks ago, vs
Person B who only got sick in Jan.
Person A will be protected for a while, because their immune system (mostly antibodies) is ramped up.
But 6 months from now, there might not be any difference.
3c. It's also worth noting that most recent evidence (bit.ly/3lgLV0S) suggests vax is still >90% effective vs hospitalization.
Even in the short term, you can't get too much better.
Even in the short term, you can't get too much better.
3d. And the US & Israel are very different in important ways:
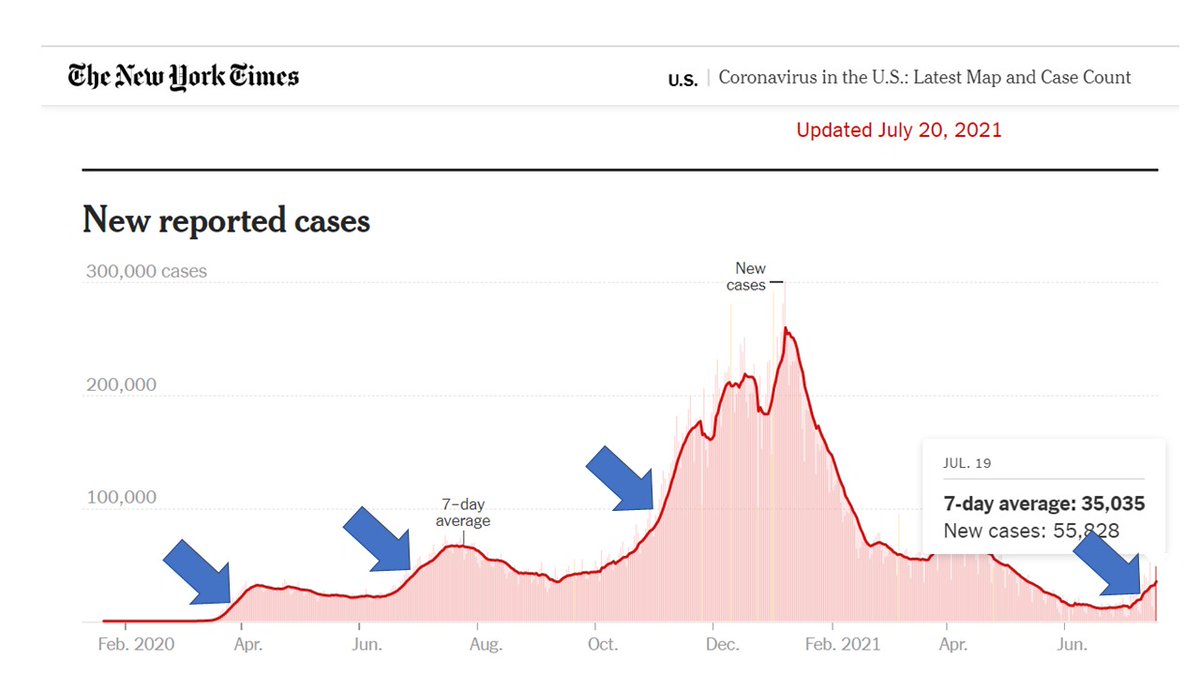
a) Israel boosters given while cases going up, but transmission in the US has fallen sharply (see below from covidestim.org).
b) Case rates in 65+ are similar to other ages in Israel, but much lower in the US.
a) Israel boosters given while cases going up, but transmission in the US has fallen sharply (see below from covidestim.org).
b) Case rates in 65+ are similar to other ages in Israel, but much lower in the US.

3e. If we want to give people a short-term boost, wouldn't it make sense to wait until cases were rising?
If we give boosters now and have another wave in Dec, we will have lost our chance to give that short-term protection when we need it most.
If we give boosters now and have another wave in Dec, we will have lost our chance to give that short-term protection when we need it most.
Bottom line, boosters in 65+:
1. Do not substantially affect transmission
2. Have no data on long-term effectiveness
3. Are best given for short-term effect when transmission is going up.
Please consider this in your $1 billion (~50 mil people * $20/dose) decision. Thank you.
1. Do not substantially affect transmission
2. Have no data on long-term effectiveness
3. Are best given for short-term effect when transmission is going up.
Please consider this in your $1 billion (~50 mil people * $20/dose) decision. Thank you.
• • •
Missing some Tweet in this thread? You can try to
force a refresh