
Let’s discuss 3 facts:
1. You and your parents before you have been managing and balancing RISK v. DOING STUFF your whole life.
2. Over time your risk of dying of COVID will shrink beneath other risks.
3. We’ve been happily killing each other with infectious diseases forever. 1/
1. You and your parents before you have been managing and balancing RISK v. DOING STUFF your whole life.
2. Over time your risk of dying of COVID will shrink beneath other risks.
3. We’ve been happily killing each other with infectious diseases forever. 1/

Like it or not (and style notwithstanding), this is the debate people like @VPrasadMDMPH and @drjohnm are trying to have right now.
And all of us will have sooner or later. 2/
And all of us will have sooner or later. 2/
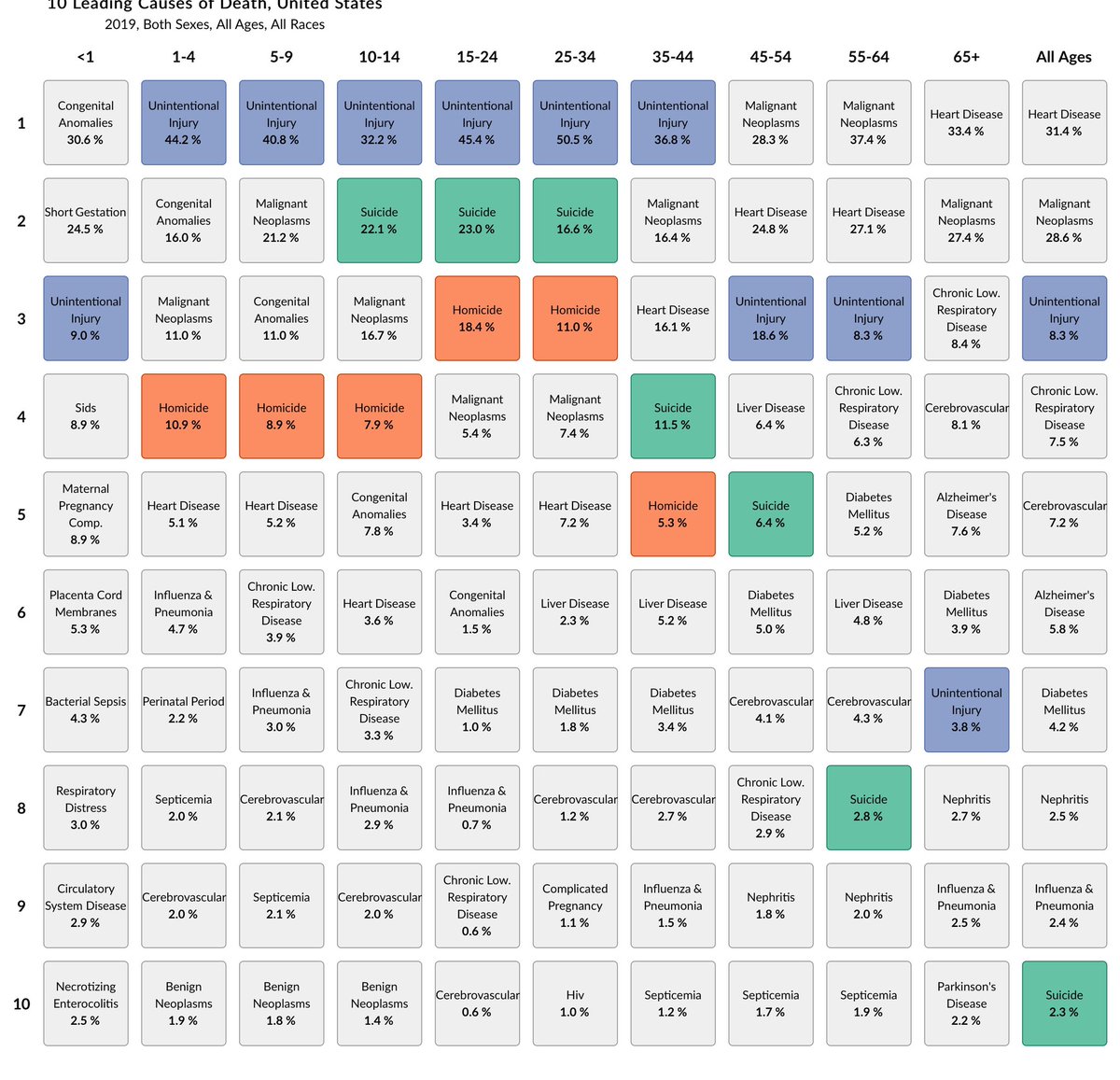
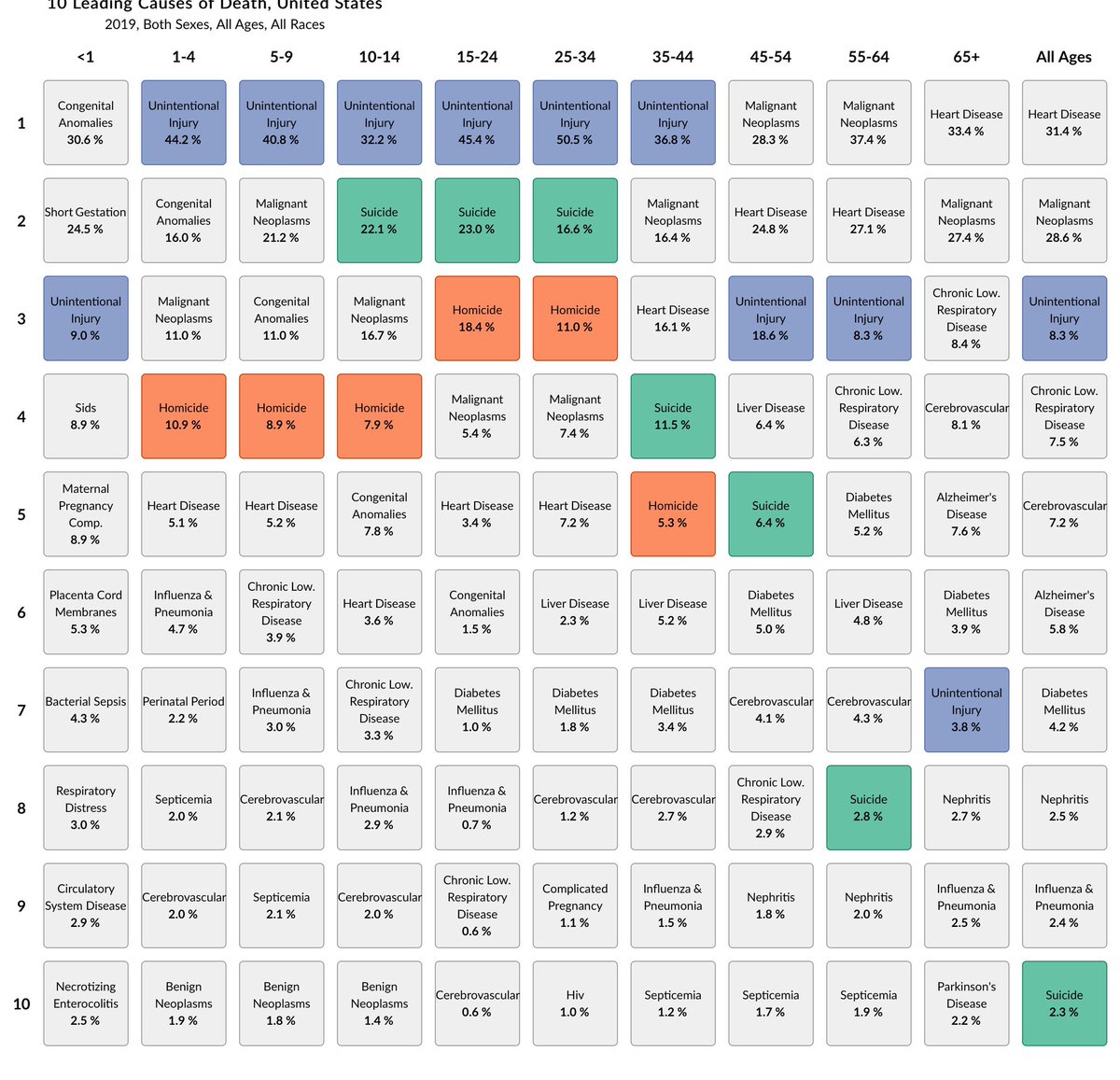
Let’s look at my column together (from @CDCgov).
I’m 45-54. You could easily reduce some of my TOP 10 risks of death by:
- outlawing cars: unintentional injury
- outlawing firearms: homicide, suicide
- outlawing tobacco and alcohol: liver/lung dz
But… 3/
I’m 45-54. You could easily reduce some of my TOP 10 risks of death by:
- outlawing cars: unintentional injury
- outlawing firearms: homicide, suicide
- outlawing tobacco and alcohol: liver/lung dz
But… 3/
We’ve already decided (especially in the US) to strike a balance between SAFETY and FREEDOM. 4/
If you work in a LEVEL 1 trauma center like me, you know people die every day because of the decisions they—and other people—make.
COVID, masks, and vaccines are not some new novel factors in public health. They are ~joining~ a million other ones. 5/
COVID, masks, and vaccines are not some new novel factors in public health. They are ~joining~ a million other ones. 5/
We already balance RISK and SAFETY in the US. If you haven’t noticed, this is not a static nor universally jolly process!!! 6/
It’s contentious and personal and always leaves a lot of people unhappy. Sometimes the MAJORITY of people. 7/
What we see in states like Florida as compared to Vermont, California or Colorado is different balance points being tested. This is okay. We have np been doing this every day of your life. 8/
It’s fun to be furious and dogmatic but the “mask nihilists” who say we should be dropping masks especially for kids are just picking a point a little bit towards facial freedom and a little bit away from safety.
It’s okay. We have to discuss the balance point. 9/
It’s okay. We have to discuss the balance point. 9/
Unlike cars, cigarettes, motorcycles, guns and they myriad of other dangerous yet fun stuff we have to balance between freedom and safety, COVID will vanish. 10/
It may not ~completely~ vanish, but it’s going to shrink beneath our other risks we love to fight about.

So in addition to picking our balance point today, we do have to anticipate a future when you can sneeze on someone on the subway or get sneezed on just like the good old days in 2017. 🤧🤧🤧 11/
In summary, calm your ass down. Leash your dogma. Stop making it personal and discuss the ISSUES not the PEOPLE.
Realize you will abandon your current stance over time if you have any brains. This chart will become accurate again in a few years. 12/
Realize you will abandon your current stance over time if you have any brains. This chart will become accurate again in a few years. 12/
• • •
Missing some Tweet in this thread? You can try to
force a refresh








