Data presented below show nearly 33% of unvaccinated adult Israeli residents were previously infected.
Why is this important & has this contributed to misinterpretation of Israeli data?
This thread wll explore these questions.
1/n
Why is this important & has this contributed to misinterpretation of Israeli data?
This thread wll explore these questions.
1/n
Israeli MoH releases periodic vaccination reports on its Telegram site. This table breaks down vaccination status by age groups as of September 14, 2021 listing total population and number given 1/2/3 doses plus those unvaccinated but recovered from previous infection
2/n
2/n
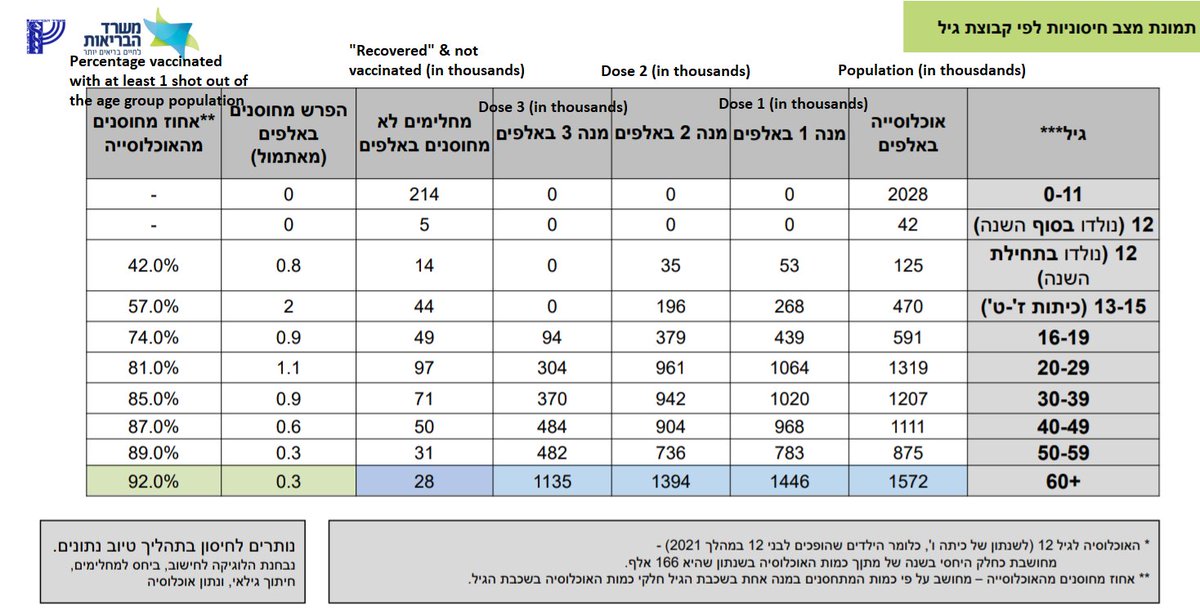
From these data, I constructed this table with % of population unvaccinated, given 1 dose, 2 doses, & 3 doses, & proportion of unvaccinated are previously infected.
Note that >30% of total unvaccinated Israelis were previously infected, & >1/3 for all age groups in 20-59yr
3/n
Note that >30% of total unvaccinated Israelis were previously infected, & >1/3 for all age groups in 20-59yr
3/n

Why does this matter? Because literature is clear they have strong immune protection even if not vaccinated (see post link below).
As a result, VE estimates will be strongly attenuated if previously infected are not removed from the unvaccinated.
4/n
covid-datascience.com/post/overwhelm…
As a result, VE estimates will be strongly attenuated if previously infected are not removed from the unvaccinated.
4/n
covid-datascience.com/post/overwhelm…
To illustrate this effect, consider a populaton of 1m, 75% vaccinated, 1/3 unvaccinated previously infected, infection rate of 0.01 for unvaccinated no previous infection, VE=65%, and previous infections reduce risk of reinfection by 90%. Here is the effect:
5/n
5/n

We see failure to remove previously infected attenuates VE from 65% to 50%. Here is the same scenario assuming VE=50%, that is attenuated to 28.6% if previously infected are not removed from unvaccinated.
6/n
6/n

This is relevant since MoH reported in late July VE reduced to 44% for vax in Feb & 16% for vax in Jan, creating impression that vaccine effectiveness was going to 0% quickly after 6m.
Their report didn’t mention if they removed previously infected.
7/n
gov.il/BlobFolder/rep…
Their report didn’t mention if they removed previously infected.
7/n
gov.il/BlobFolder/rep…
Three rigorous studies were done (Mizrahi et al,Israel et al,Goldberg et al) on waning immunity – all removed previously infected & adjusted for confounders as much as possible. Here is the Goldberg paper that also compared with unvaccinated controls.
8/n
medrxiv.org/content/10.110…
8/n
medrxiv.org/content/10.110…
These all found 1.6-2.2x reduction in VE from those vaccinated in Jan-Feb vs. Apr-May, but relative to unvaccinated, VE reduced from 75-80% to 50-65%., much higher than the 44%/16% MoH reported
Is it possible MoH report mistakenly left previously infected in unvaccinated?
9/n
Is it possible MoH report mistakenly left previously infected in unvaccinated?
9/n
Since Israel made vax optional for previously infected and then only gave 1 dose, this especially affects the unvaccinated group. Other places, there could be some subset of “fully vaccinated” who were also previously infected and have extra protection.
10/n
10/n
For this reason, all locales should, whereever possible, split out data not just by vaccination status but also previous infection status.
And we should all be mindful of this potential effect when evaluating simple analyses to estimate VE.
11/n
And we should all be mindful of this potential effect when evaluating simple analyses to estimate VE.
11/n
BTW thanks to Nurit Baytch who sent me link to MOH methodology document showing in their analyses they DO remove unvaccinated from the strata before estimating VE: t.me/MOHreport/8321
... hopefully they did that for this waning immunity analysis: gov.il/BlobFolder/rep…
• • •
Missing some Tweet in this thread? You can try to
force a refresh