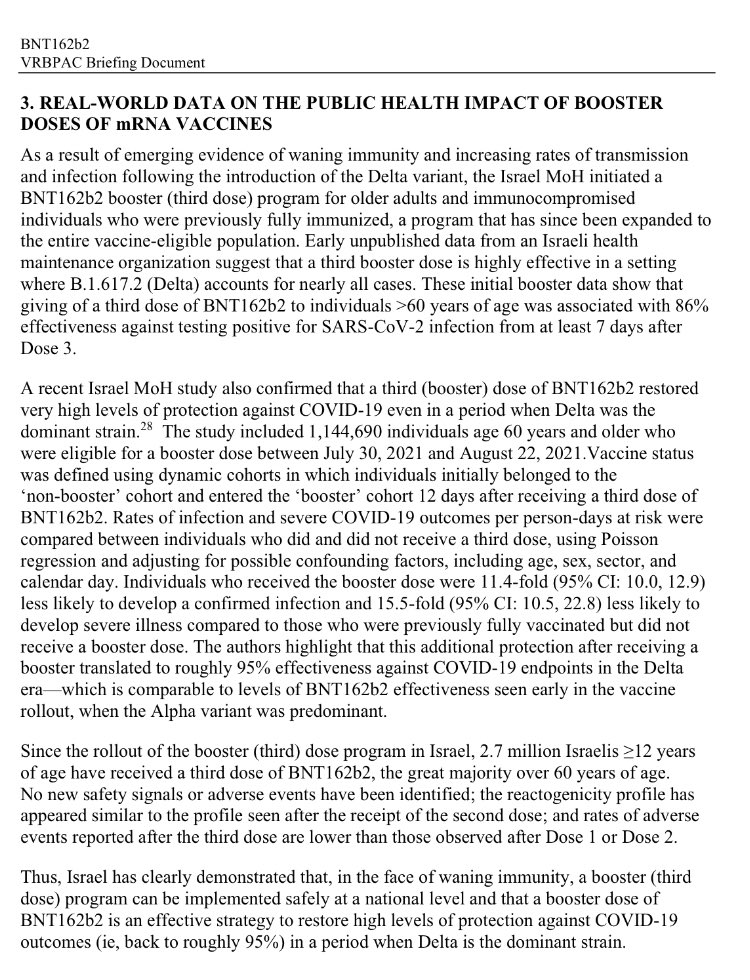
Here's the NEJM study of the data. A few thoughts
1) Big risk rate differences but dataset appears to lack behavioral/social data that would help identify potential confounders related to differences in exposure/viral dose at exposure
nejm.org/doi/full/10.10…
1) Big risk rate differences but dataset appears to lack behavioral/social data that would help identify potential confounders related to differences in exposure/viral dose at exposure
nejm.org/doi/full/10.10…
2) Lacks safety outcome data, so hard to discuss risks vs. benefits
3) Use of time period to set lower bound of effect is questionable. Behavioral differences related to the time periods, and how they shift, are much more of an unknown and are historically contingent. 
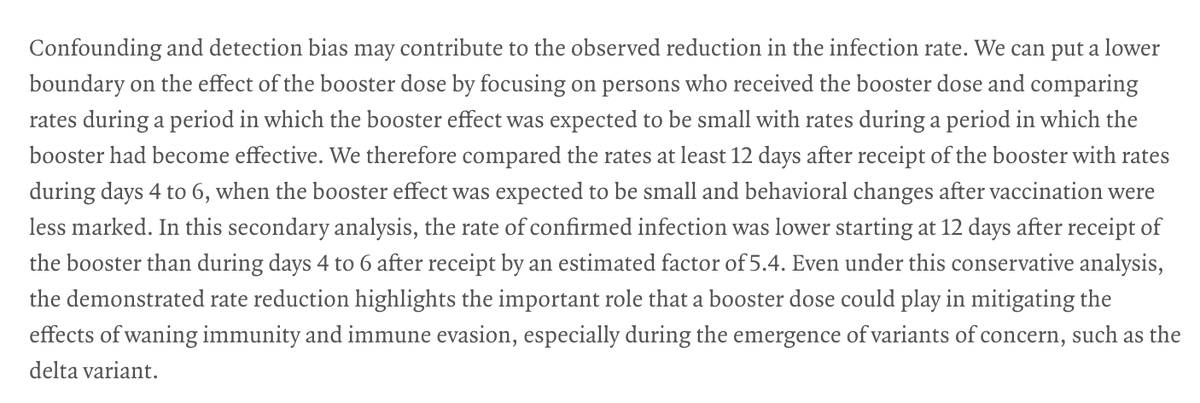
4) Authors neglect biases related to exposure risk beyond "cautiousness."
Cautiousness = masking, distancing
Other exposure risks = social communities (beyond home geographic area controlled for)
No good data/analysis to deal with much of these.
Cautiousness = masking, distancing
Other exposure risks = social communities (beyond home geographic area controlled for)
No good data/analysis to deal with much of these.
5) Irresponsible public communication of rate difference describing it as or implying it to be *fully* the effect of boosters.
It is essential at this moment to either educate public on confounding or to at least not falsely suggest such large effects.
It is essential at this moment to either educate public on confounding or to at least not falsely suggest such large effects.
• • •
Missing some Tweet in this thread? You can try to
force a refresh