
Tox ECGs CAN be made easy 💊💊💊
Understanding these ECG changes make them easier to recognise 👇
Understanding these ECG changes make them easier to recognise 👇
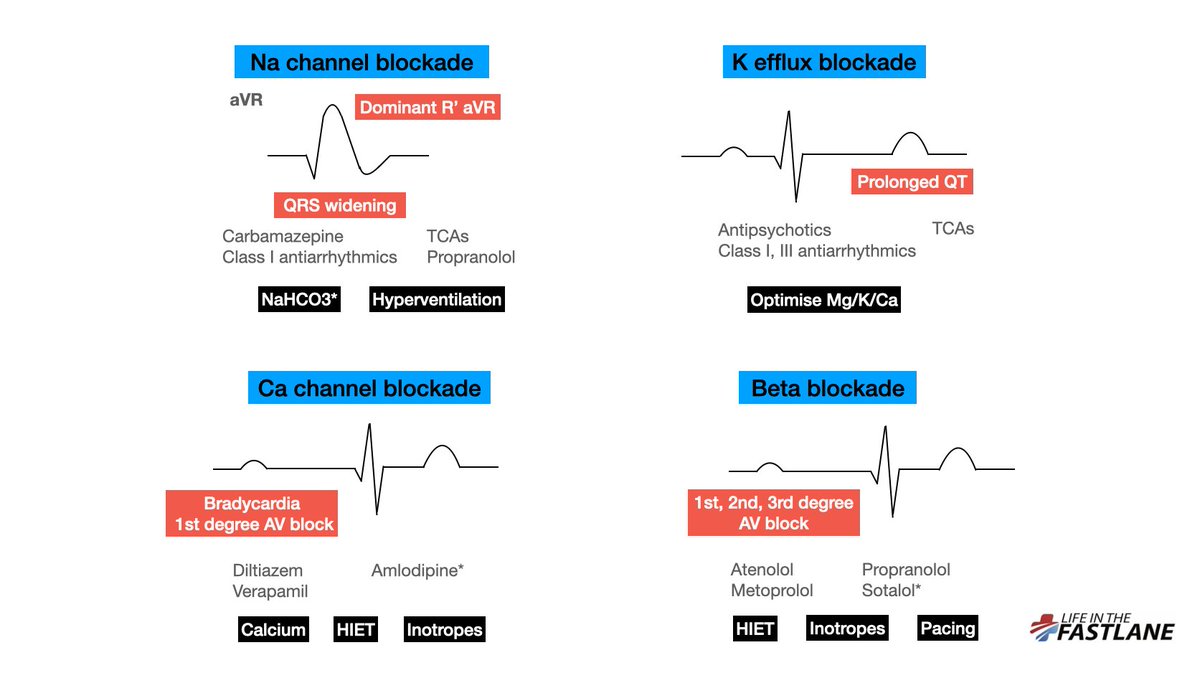
@LITFLblog We may have heard that Na channel blockade causes “right axis deviation of the terminal QRS”.
But what does this actually mean? (1/13)
But what does this actually mean? (1/13)
Well, the right-sided intraventricular conduction system is more susceptible to Na channel blocker toxicity than the left.
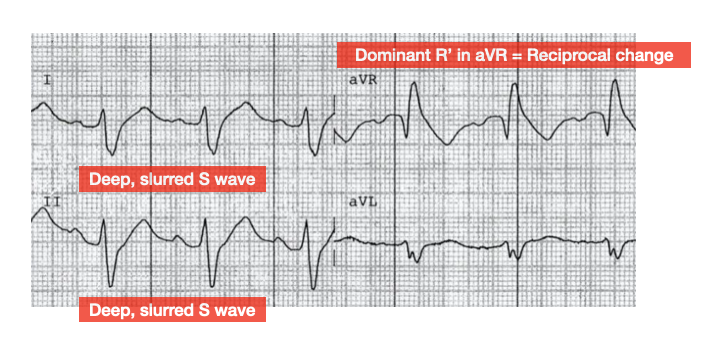
This leads to delayed depolarization of the RV. As is the case in RBBB, delayed RV conduction manifests as deep, slurred S waves in leads I, II, V5-6 (2/13)
This leads to delayed depolarization of the RV. As is the case in RBBB, delayed RV conduction manifests as deep, slurred S waves in leads I, II, V5-6 (2/13)
aVR is not a real lead – it is calculated from leads I and II and is a mirror (reciprocal) image of changes seen in these leads (3/13):
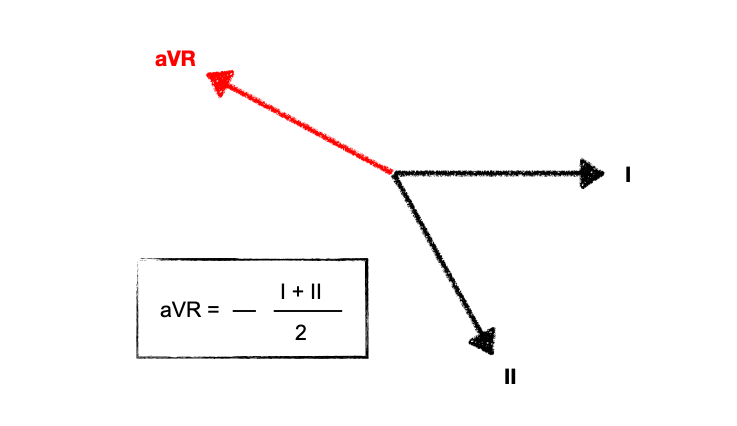
Deep, slurred S waves of delayed RV conduction are thus reflected as a dominant R’ wave in aVR.
The “amplitude” of R’ in aVR is mentioned frequently, but actually the pattern recognition of a widened R wave is just as important. (4/13)
The “amplitude” of R’ in aVR is mentioned frequently, but actually the pattern recognition of a widened R wave is just as important. (4/13)
With worsening toxicity, left-sided conduction pathways are increasingly affected, eventually leading to a “sine wave” appearance reminiscent of hyperkalaemia
Patients are at increased risk of ventricular dysrhythmias with QRS > 100ms, and of seizures with QRS > 160ms. (5/13)
Patients are at increased risk of ventricular dysrhythmias with QRS > 100ms, and of seizures with QRS > 160ms. (5/13)
NaHCO3 can improve conduction delay with resultant shortening of QRS.
However, there can be a variable response to this. Do not continue to give repeated boluses unless there is a clear response. There have been case reports of death from this. (6/13)
However, there can be a variable response to this. Do not continue to give repeated boluses unless there is a clear response. There have been case reports of death from this. (6/13)
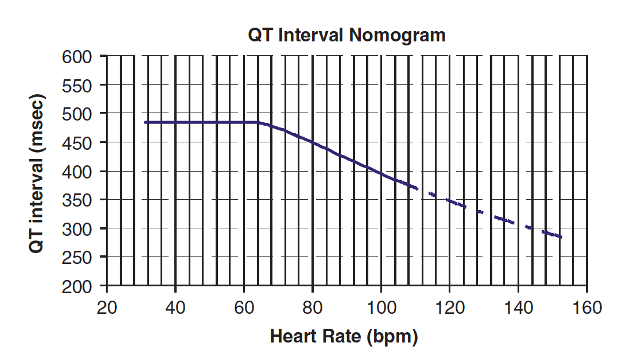
A reminder on measuring the QT interval. Don’t rely on the computer.
The biggest pitfall of computer interpretation is including separate U waves in calculations, which leads to falsely high measurements of 600ms +. (7/13)
The biggest pitfall of computer interpretation is including separate U waves in calculations, which leads to falsely high measurements of 600ms +. (7/13)

There is no specific correct lead to measure – simply use the lead with the longest interval. The general recommendation to measure II or V5-6 comes from the fact that these leads usually correlate to the overall vector of depolarisation. (8/13)
In tox ECGs, the absolute value can measured and plotted on the nomogram to predict if patients are at risk of TdP (Torsades de Pointes).
Use this as opposed to QTc (9/13)
Use this as opposed to QTc (9/13)
Amlodipine is a dihydropyridine with higher affinity for peripheral Ca channels. This leads to vasoplegia with BP 👇 and initial reflex HR 👆
NA/NE is the initial BP support option. However, at high doses selectivity 👇 and there is concurrent effects on cardiac channels (10/13)
NA/NE is the initial BP support option. However, at high doses selectivity 👇 and there is concurrent effects on cardiac channels (10/13)
First degree AV block is the first sign of beta blocker toxicity and usually manifests BEFORE bradycardia. Do not be falsely reassured by a normal heart rate.
Sotalol also has class III (AP prolonging) actions, leading to QT prolongation and a risk of TdP. (11/13)
Sotalol also has class III (AP prolonging) actions, leading to QT prolongation and a risk of TdP. (11/13)
Lastly, digoxin needs an infographic of it’s own. Na/K ATPase blockade predisposes to a multitude of arrhythmias due to increased automaticity and decreased AV conduction.
Think of it as a combination of excitant ☕️ and suppressant 😴 activity. (12/13)
Think of it as a combination of excitant ☕️ and suppressant 😴 activity. (12/13)

*HIET = high-dose insulin euglycemic therapy.
Best used in conjunction with inotropes, HIET allows the heart to overcome the “metabolic starvation” caused by CCB (and beta-blocker) toxicity.
@precordialthump gives a great overview here: litfl.com/high-dose-insu… (13/13)
Best used in conjunction with inotropes, HIET allows the heart to overcome the “metabolic starvation” caused by CCB (and beta-blocker) toxicity.
@precordialthump gives a great overview here: litfl.com/high-dose-insu… (13/13)
• • •
Missing some Tweet in this thread? You can try to
force a refresh


