
Ok, a tweetorial for the most frequently asked question of this period for all virologists: what will flu do.
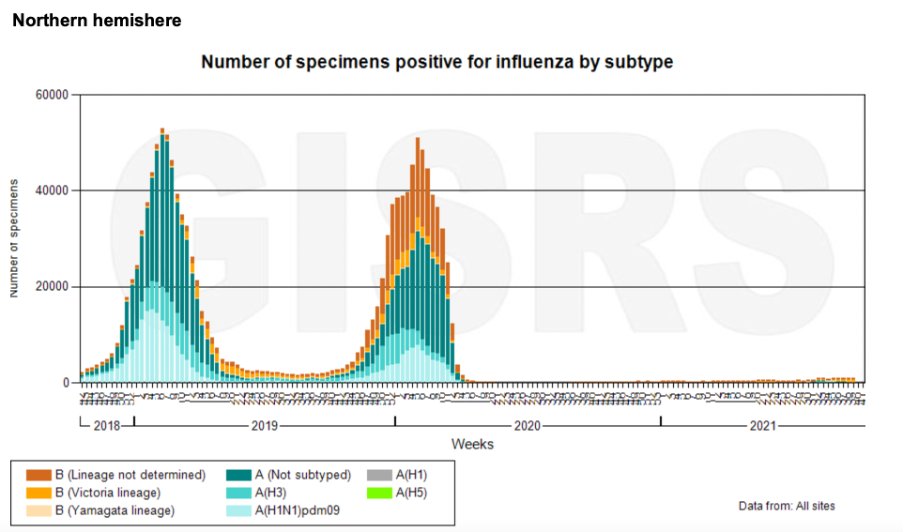
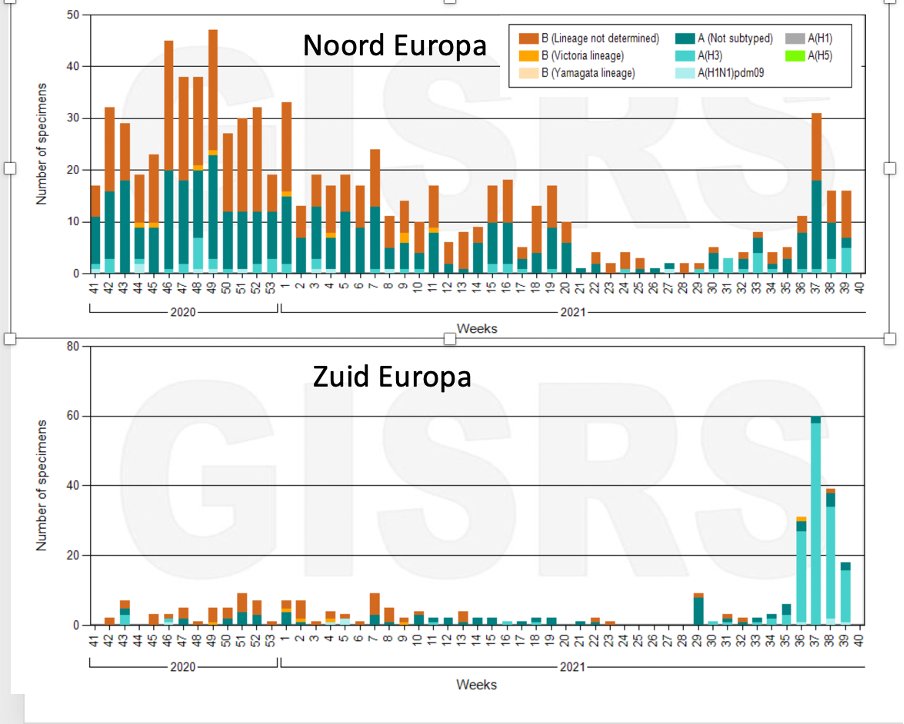
I was asked to present how we look at flu in the coming season. First question: what will the COVID 19 pandemic “do” in fall. Restrictions to reduce circulation have really had an impact on flu circulation as well. Look at the global flu surveillance data who.int/tools/flunet 
Then question: what happens if there is a two year gap in flu circulation? What does that do to population immunity? This study looked at waning of protective antibodies over time, and estimates 25% reduction over 2 years in unvaccinated individuals.
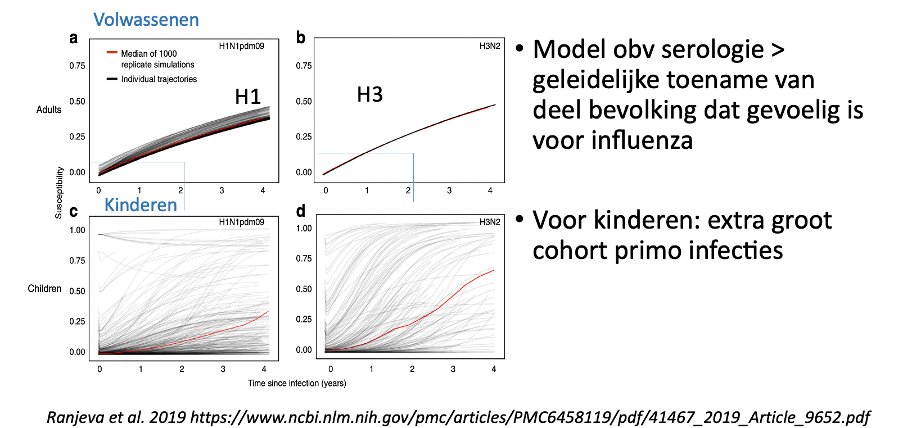
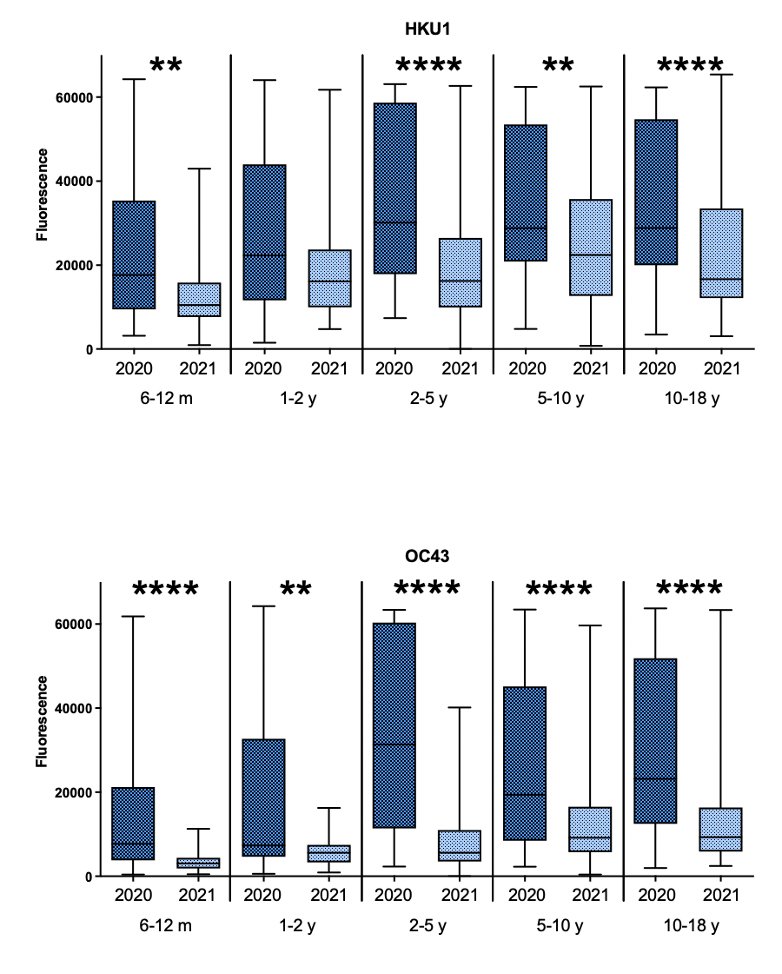
A specific question is what the role of children will be. There is a large group of young children that has not yet experienced flu. This is measurable, reduced antibodies to some seasonal respiratory viruses in children April 2020 and April 2021 (Sikkema et al)
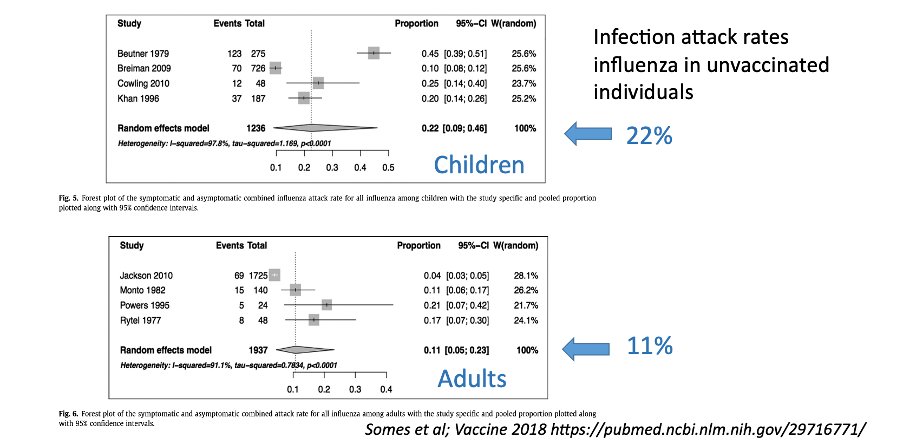
Next question: what is the infection attack ate in a typical flu season (obviously if there are no measures in place for COVID) . This study estimates 1/5 in children and 1/10 in adults
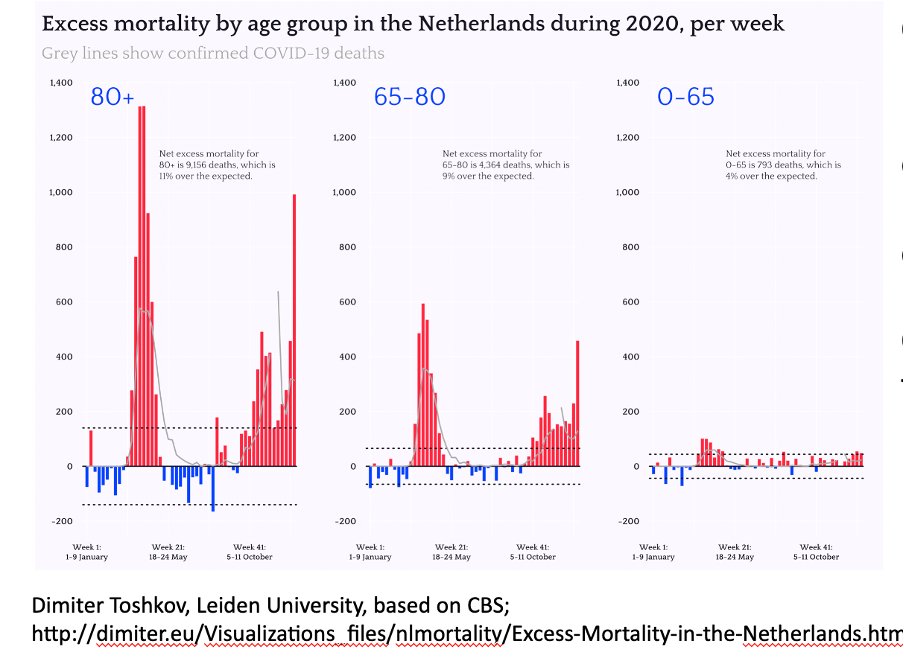
Uncertain; we have seen substantial excess mortality in the oldest age groups that also are at highest risk for severe flu. Will that result in lower flu impact in the same group?
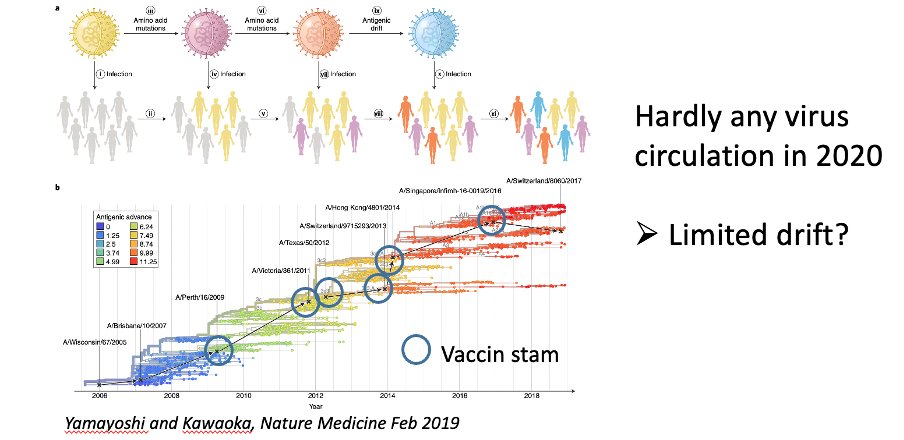
Then there is the question: which strains will circulate. This is assessed based on surveillance data but there is a gap there too, globally. On the other hand, without much virus circulation, one does not expect a lot of drift, so that works for us I think
So in all, many uncertainties. We do see that flu circulation is starting in Europe, so should be prepared
Note that this data is collected from a network of national influenza centers across the world, that share data on a weekly basis with WHO. In our country, this is a collaboration between @RIVM and @NIVEL and @ErasmusMC. We have a weekly newsletter for wo is interested

@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh



