#EACTS2021
Abstract session on Hot Topics in Transcatheter Therapies
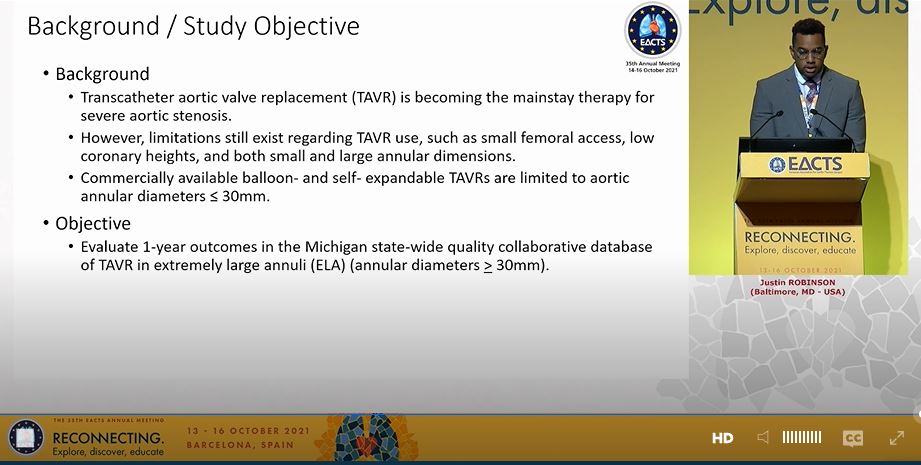
Presentation from Dr Justin Robinson on use of TAVI in patients with very large aortic annuli - Results from the Michigan TAVI Quality Collaborative
Abstract session on Hot Topics in Transcatheter Therapies
Presentation from Dr Justin Robinson on use of TAVI in patients with very large aortic annuli - Results from the Michigan TAVI Quality Collaborative
#EACTS2021
Methods here: just over 200 patients with aortic annuli in excess of the normal ranges for both the Edwards Sapien and Medtronic Corevalve systems
Methods here: just over 200 patients with aortic annuli in excess of the normal ranges for both the Edwards Sapien and Medtronic Corevalve systems

#EACTS2021
This was not easy to read. Key data here:
Mean STS score ~5%
Device success ~95%
Pacemaker - 6% Sapien 3 vs 11% Corevalve (p<0.05)
In-hosp mortality ~2%
This was not easy to read. Key data here:
Mean STS score ~5%
Device success ~95%
Pacemaker - 6% Sapien 3 vs 11% Corevalve (p<0.05)
In-hosp mortality ~2%

#EACTS2021
Significantly more mild or moderate PVL with Corevalve system at 30days, which was the same as Sapien system by 1 year
Significantly lower mean gradient with Corevalve system at 30days, same as Sapien 3 by 1 year
Significantly more mild or moderate PVL with Corevalve system at 30days, which was the same as Sapien system by 1 year
Significantly lower mean gradient with Corevalve system at 30days, same as Sapien 3 by 1 year

#EACTS2021
Limitation of this study is reliance on the TVT database - what I was not clear about is why these patients could not have surgery. Anyway, one assumes there was an MDT discussion in each case and surgery was not deemed feasible?
@GilbertTangMD
Limitation of this study is reliance on the TVT database - what I was not clear about is why these patients could not have surgery. Anyway, one assumes there was an MDT discussion in each case and surgery was not deemed feasible?
@GilbertTangMD

#EACTS2021
I think that was a point the panel were keen to make, that a single retrospective study could not be used to suggest that TAVI in very large annuli is 'ready for prime time', but that these important results do give some confidence if a patient cannot undergo surgery
I think that was a point the panel were keen to make, that a single retrospective study could not be used to suggest that TAVI in very large annuli is 'ready for prime time', but that these important results do give some confidence if a patient cannot undergo surgery

• • •
Missing some Tweet in this thread? You can try to
force a refresh