Hey #EPeeps !
Routine ICD remote check. What's going on? Patient is asymptomatic. What to do about it?
Routine ICD remote check. What's going on? Patient is asymptomatic. What to do about it?
Well, it looks like this image ⬆️ was worthwhile posting. Lots of great guesses, few correct replies. Let's get into it! (short thread)
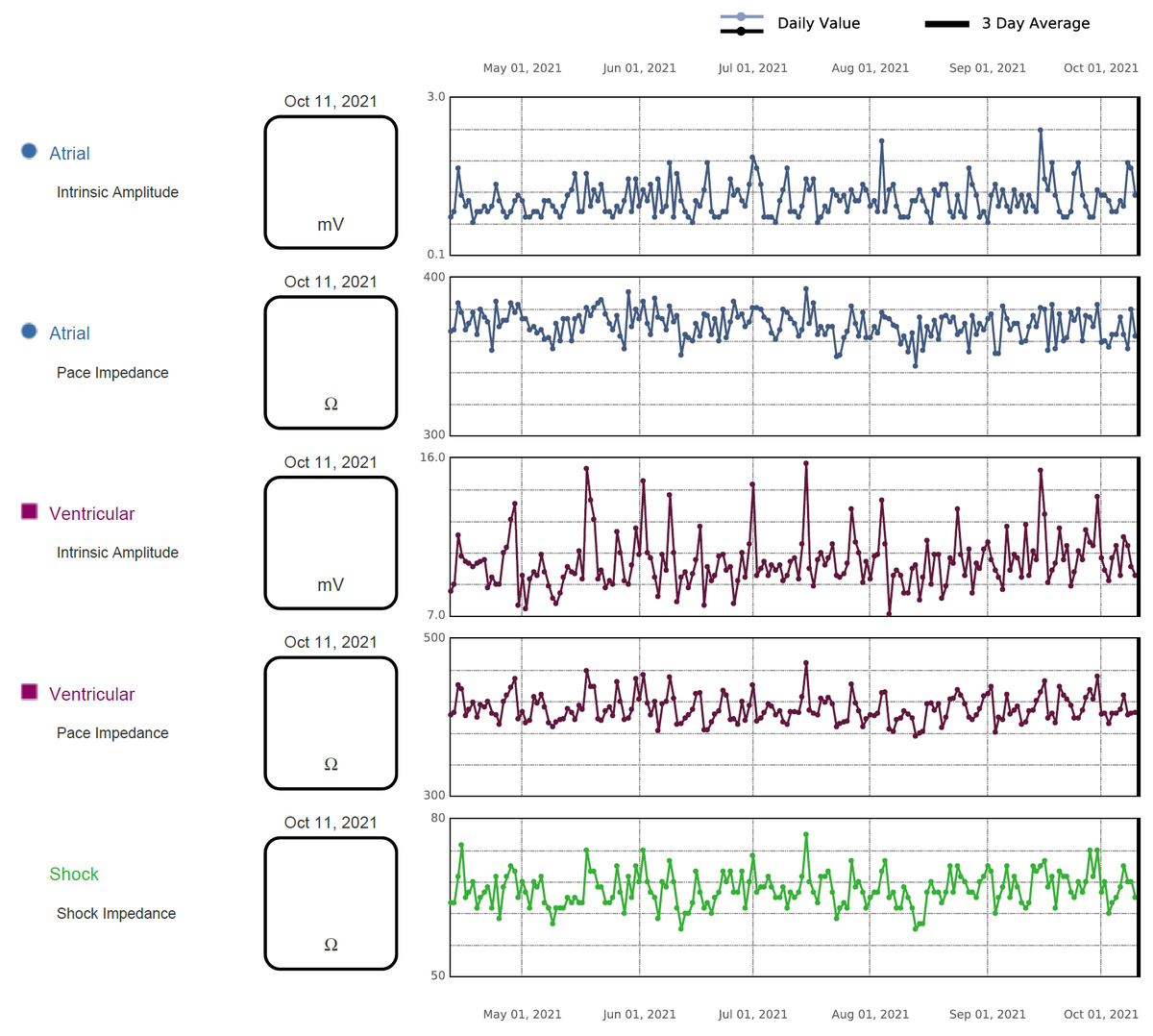
First off, here are the impedances in the leads, the programming, and another example of the noise phenomenon. 1/n
First off, here are the impedances in the leads, the programming, and another example of the noise phenomenon. 1/n


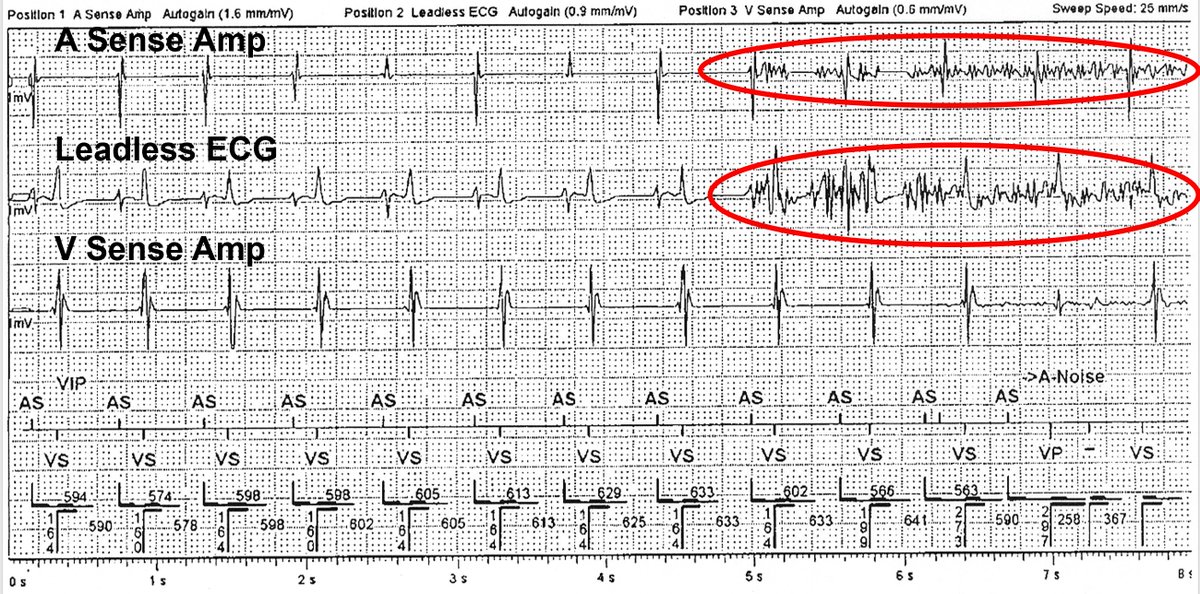
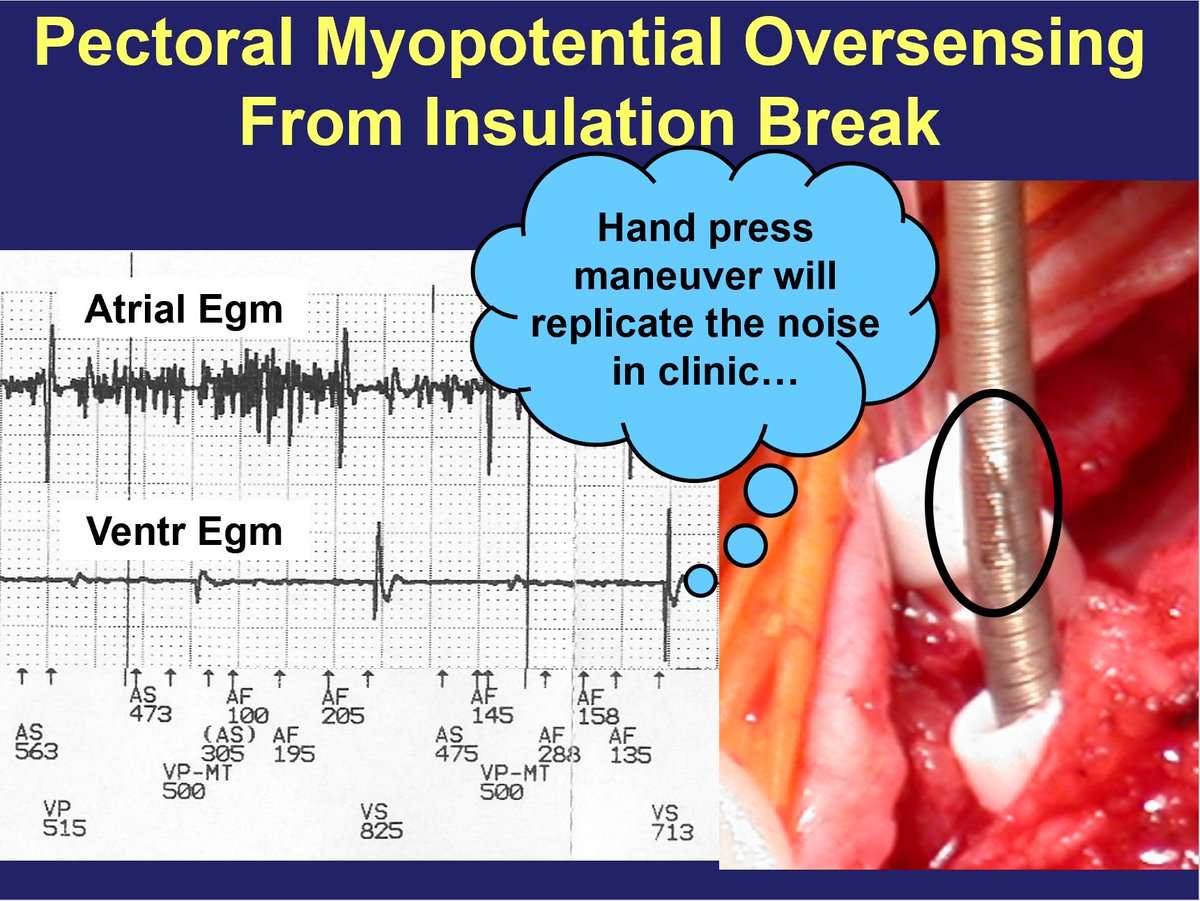
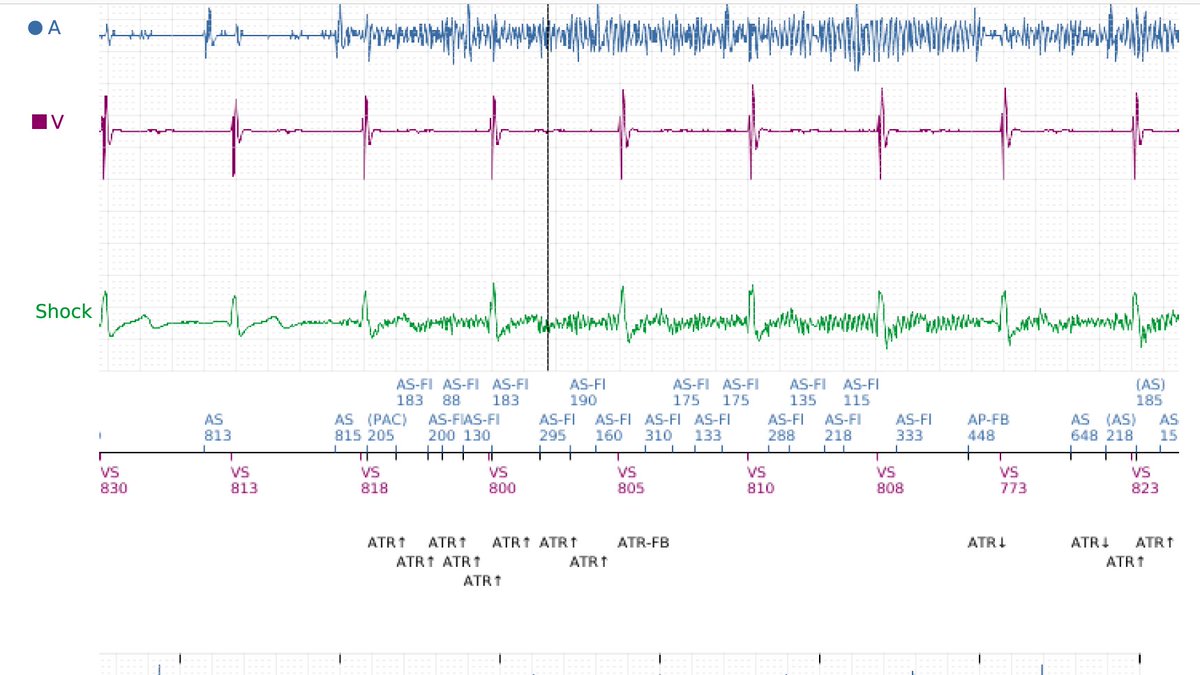
Here are some other patient examples of the same phenomenon, which show very high frequency noise on the atrial lead as well as (simultaneously) in the shock egm. Noise does *not* occur in the v.pace/sense channel (and therefore there is no ventricular oversensing seen). 2/n

There are different types of noise which can often be differentiated by morphology, pattern, & impacted egm channel(s).
External noise (EMI) is seen on all channels & the morphology/timing is usually indicative of the source. e.g. Cautery. 60Hz wall current. Tens unit. MRI . 3/n
External noise (EMI) is seen on all channels & the morphology/timing is usually indicative of the source. e.g. Cautery. 60Hz wall current. Tens unit. MRI . 3/n




Noise on a single channel also has many causes, usually with a characteristic morphology.
Lead fracture: sharp, chaotic, intermittent
Myopotentials: high frequency, shorter duration for phrenic, longer duration for pectoral
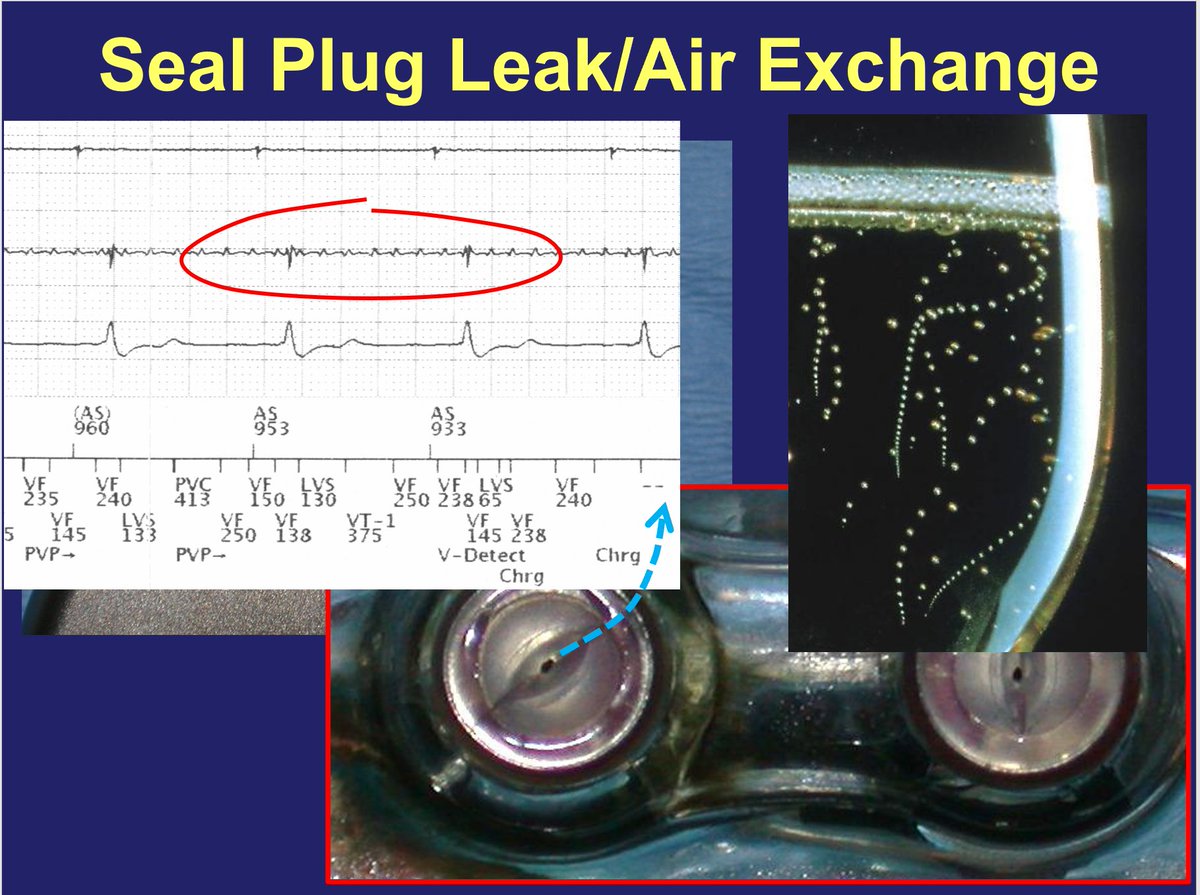
Seal plug: low amplitude punctate, <24h post-op
4/n
Lead fracture: sharp, chaotic, intermittent
Myopotentials: high frequency, shorter duration for phrenic, longer duration for pectoral
Seal plug: low amplitude punctate, <24h post-op
4/n


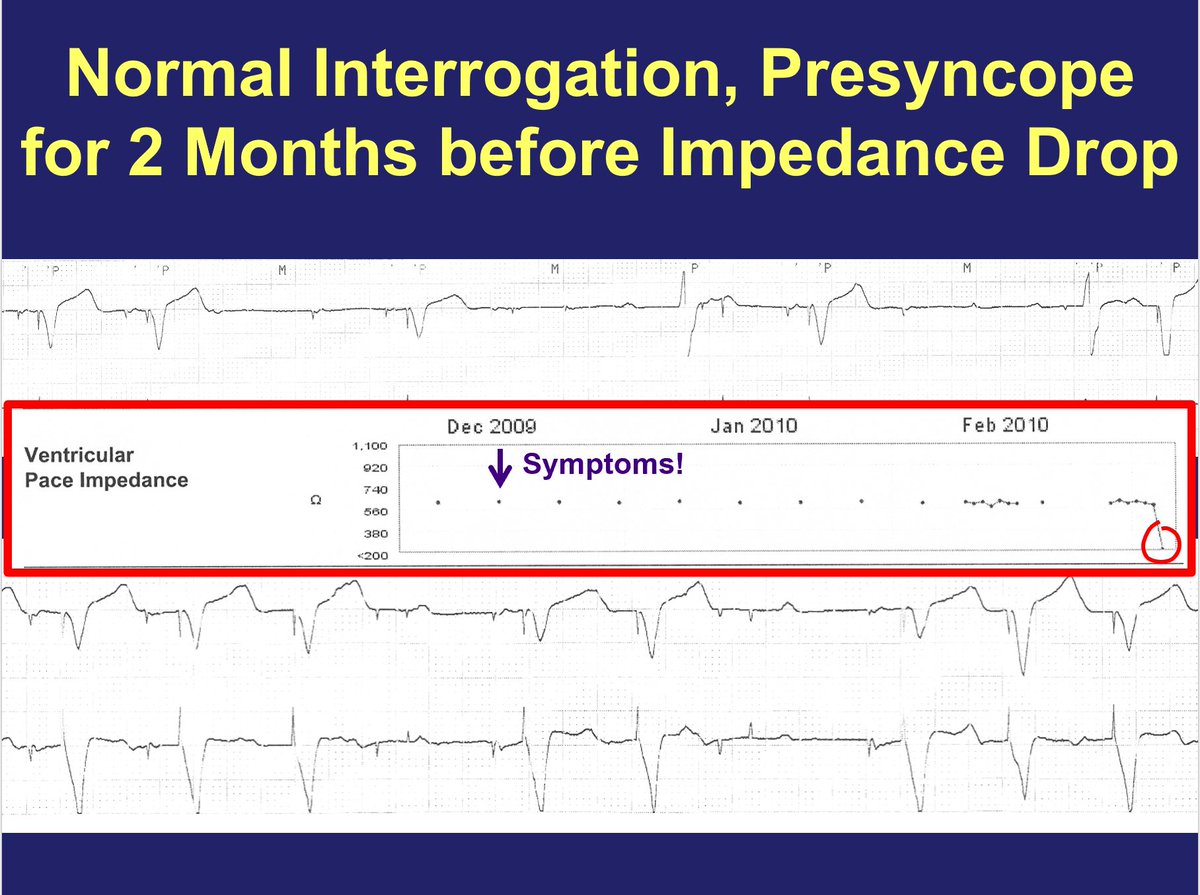
Lead fracture is associated with a sudden *rise* in impedance (slow rise = tip fibrosis)
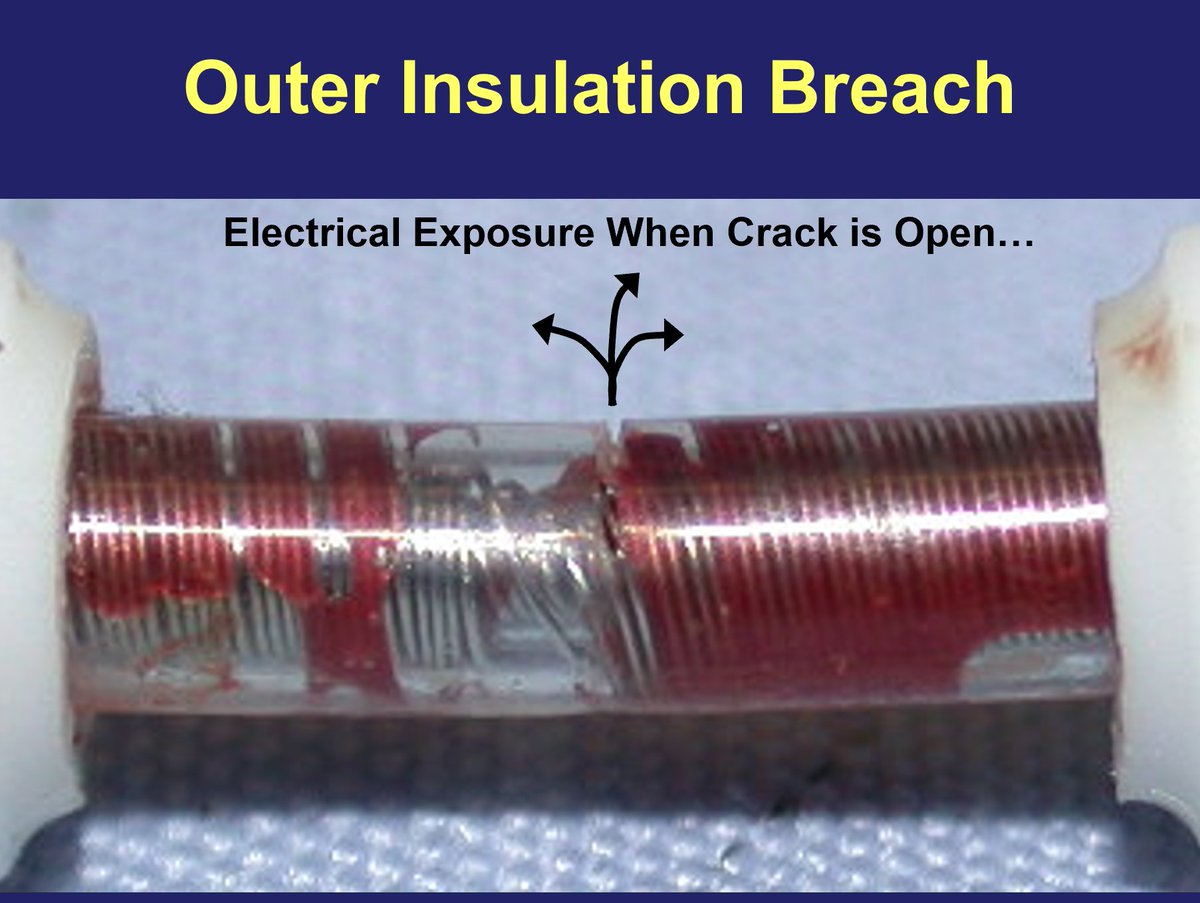
Insulation break is associated with a *drop* in impedance.
A *lack* of impedance change does not necessarily indicate absence of lead issue - impedance change may not show up right away.
5/n
Insulation break is associated with a *drop* in impedance.
A *lack* of impedance change does not necessarily indicate absence of lead issue - impedance change may not show up right away.
5/n


In this case, absence of noise in RV pace/sense rules out external EMI.
Morphology of noise in a.lead suggests myopotential oversensing which almost always is pectoral muscle sensing due to insulation break at the pocket.
Absence of impedance drop is common if breach is small 6/n
Morphology of noise in a.lead suggests myopotential oversensing which almost always is pectoral muscle sensing due to insulation break at the pocket.
Absence of impedance drop is common if breach is small 6/n

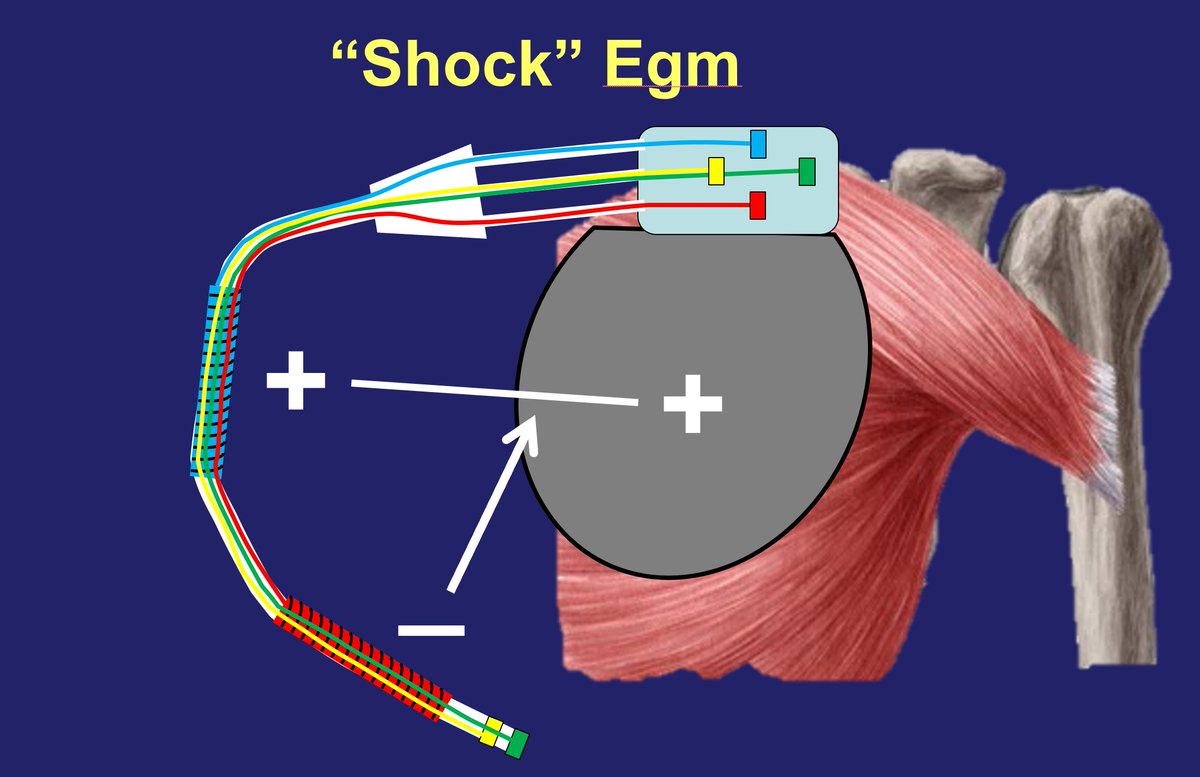
So what is going on with the shock egm?
The "Shock" or "Far-Field" or "Leadless ECG" channel uses the device itself as one of the electrodes in sensing (just like unipolar pacemaker sensing). As such, pectoral muscle contraction will be sensed - this is normal behavior. 7/n
The "Shock" or "Far-Field" or "Leadless ECG" channel uses the device itself as one of the electrodes in sensing (just like unipolar pacemaker sensing). As such, pectoral muscle contraction will be sensed - this is normal behavior. 7/n
This phenomenon used to go unnoticed, but comes to attention more often in the office with the advent of wireless device communication (can see this "noise" on shock egm while pt getting up on the exam table, without the wand in place). Can show with hand press maneuver 8/n


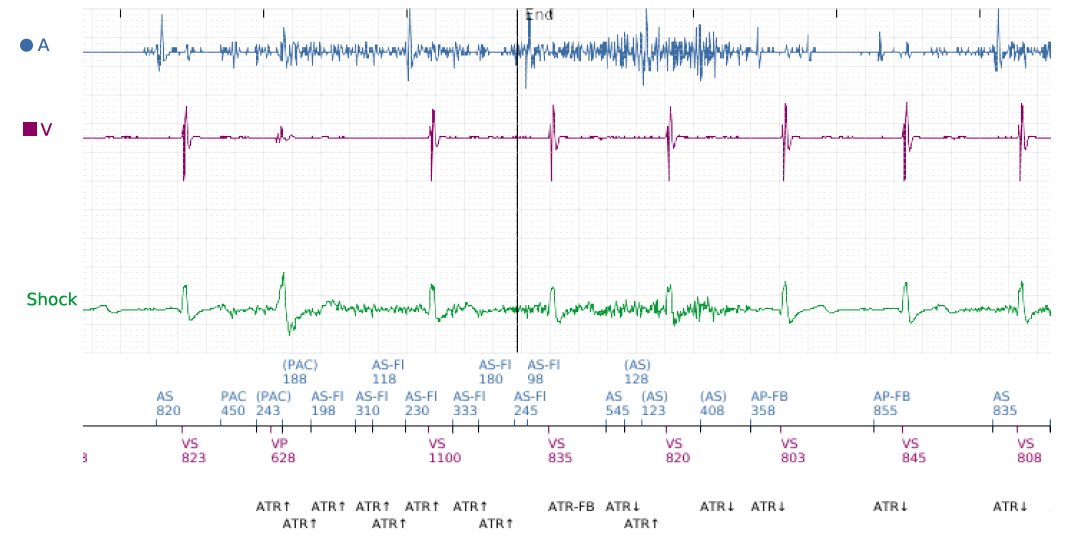
The other scenario where shock egm myopotentials come to attention is in stored egm events where pectoral myopotentials are oversensed, such as false AHR events from a.lead insulation break. Event egms show myopotentials in Atrial & shock egm, the latter being incidental. 9/n
So the best explanation for the event is a small atrial lead insulation break that hasn't yet resulted in impedance drop, leading to pectoral muscle oversensing & false ATR events. Shock egm signals shouldn't be interpreted as any problem with v.lead - it's a normal finding. 10/n
Main consequences of this are benign.
➡️False ATR events (could potentially obscure real a.fib events by "filling up" log with false events)
➡️Brief tracking/v.pacing of noise (few ways to program device to reduce this phenomenon)
➡️Often can wait until gen change to address
End.
➡️False ATR events (could potentially obscure real a.fib events by "filling up" log with false events)
➡️Brief tracking/v.pacing of noise (few ways to program device to reduce this phenomenon)
➡️Often can wait until gen change to address
End.
• • •
Missing some Tweet in this thread? You can try to
force a refresh