
#IssaTweetorials
#EPeeps
Impedance & RF ablation:
Part 1: How does impedance affect RF lesion formation?
1/8
During RF ablation, system impedance = impedance of genera¬tor + transmission lines + catheter + electrode-tissue interface + skin patch interface + interposed tissues.
#EPeeps
Impedance & RF ablation:
Part 1: How does impedance affect RF lesion formation?
1/8
During RF ablation, system impedance = impedance of genera¬tor + transmission lines + catheter + electrode-tissue interface + skin patch interface + interposed tissues.

2/8
IMPEDANCE & POWER
The magnitude of RF current delivered by the generator is determined by impedance btwn ABL electrode and ground pad. Ablation at lower impedance yields higher current output (and tissue heating) compared with ablation at a similar power & higher impedance.
IMPEDANCE & POWER
The magnitude of RF current delivered by the generator is determined by impedance btwn ABL electrode and ground pad. Ablation at lower impedance yields higher current output (and tissue heating) compared with ablation at a similar power & higher impedance.

3/8
IMPEDANCE OF ELECTRICAL CONDUCTORS
Currently used electrical conductors from the generator to the patient and from the ground pad back to the generator are designed to have low electrical resistance to help minimize power loss within those conductors.
IMPEDANCE OF ELECTRICAL CONDUCTORS
Currently used electrical conductors from the generator to the patient and from the ground pad back to the generator are designed to have low electrical resistance to help minimize power loss within those conductors.

4/8
IMPEDANCE AT SKIN-GROUND PAD INTERFACE
Part of the RF power is dissipated at the skin-ground pad interface. High impedance at that location results in more RF power loss and skin heating at the ground pad, and less energy available for myocardial heating at ABL electrode.
IMPEDANCE AT SKIN-GROUND PAD INTERFACE
Part of the RF power is dissipated at the skin-ground pad interface. High impedance at that location results in more RF power loss and skin heating at the ground pad, and less energy available for myocardial heating at ABL electrode.

5/8
IMPEDANCE AT SKIN-GROUND PAD INTERFACE
A large ground pad surface area (or adding a second patch) and meticulous skin preparation to optimize skin contact are required at to reduce impedance and minimize power loss, and to effectively dissipate heat and prevent skin burns.
IMPEDANCE AT SKIN-GROUND PAD INTERFACE
A large ground pad surface area (or adding a second patch) and meticulous skin preparation to optimize skin contact are required at to reduce impedance and minimize power loss, and to effectively dissipate heat and prevent skin burns.

6/8
IMPEDANCE AT ELECTRODE-BLOOD-TISSUE INTERFACE
With ABL electrode in contact with the endocardial wall, part of the electrode contacts tissue and the rest contacts blood, and the RF current flows through both myocardium & blood, then through the thorax to the ground pad.
IMPEDANCE AT ELECTRODE-BLOOD-TISSUE INTERFACE
With ABL electrode in contact with the endocardial wall, part of the electrode contacts tissue and the rest contacts blood, and the RF current flows through both myocardium & blood, then through the thorax to the ground pad.

7/8
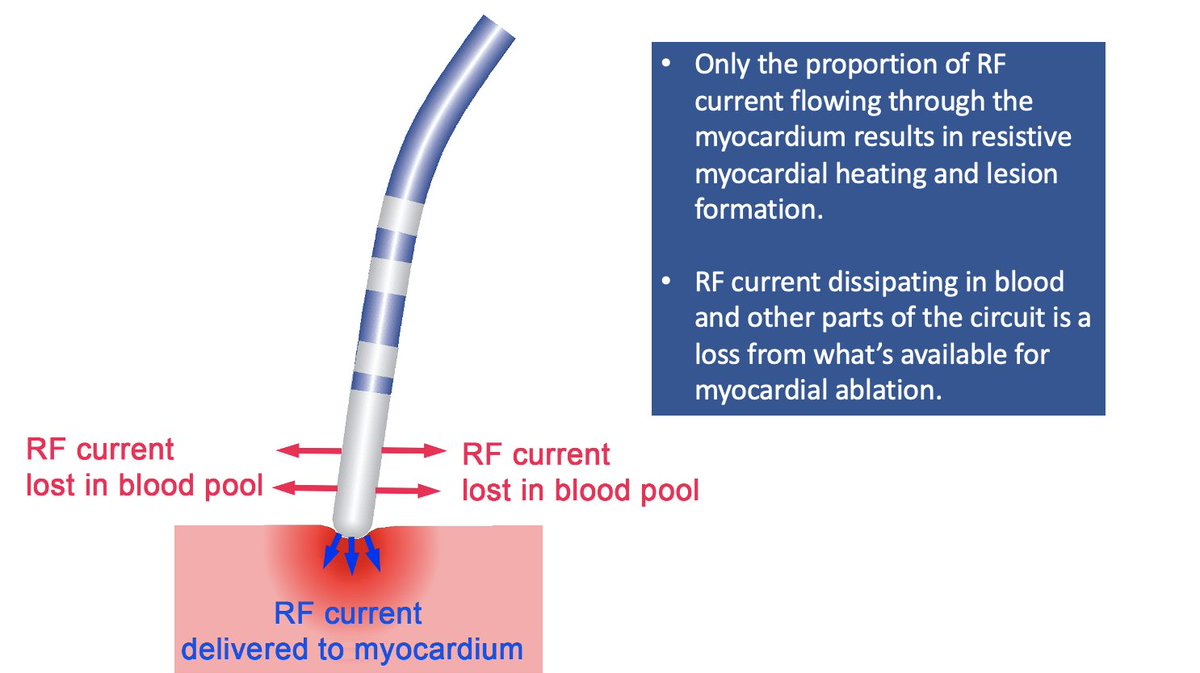
RF LESION FORMATION
With normal electrode-tissue contact, only a fraction of all power is effectively applied to the tissue. The rest is dissipated in the blood pool and elsewhere in the patient.
RF LESION FORMATION
With normal electrode-tissue contact, only a fraction of all power is effectively applied to the tissue. The rest is dissipated in the blood pool and elsewhere in the patient.
8/8
MODULATING IMPEDANCE TO IMPROVE RF LESION FORMATION
RF current flow into the myocardium can be increased by reducing total circuit impedance and by modulating the ratios of electric impedances between RF electrode, blood pool, and cardiac tissue.
MODULATING IMPEDANCE TO IMPROVE RF LESION FORMATION
RF current flow into the myocardium can be increased by reducing total circuit impedance and by modulating the ratios of electric impedances between RF electrode, blood pool, and cardiac tissue.




• • •
Missing some Tweet in this thread? You can try to
force a refresh




















