
ORAL ANTIVIRALS (e.g. molnupiravir and now "Paxlovid"): Why is everyone so excited about designated antivirals that target enzymes involved in the viral lifecycle of SARS-CoV-2? Because they will directly treat COVID & hopefully prevent severe disease
smithsonianmag.com/science-nature…
smithsonianmag.com/science-nature…
So, what is the lifecycle of the virus & where do these antivirals work? Good article on lifecycle, showing various steps how SARS-CoV-2 enters the cell & replicates. There is a polymerase called the viral RNA-dependent RNA polymerase and a viral protease
nature.com/articles/s4157…
nature.com/articles/s4157…
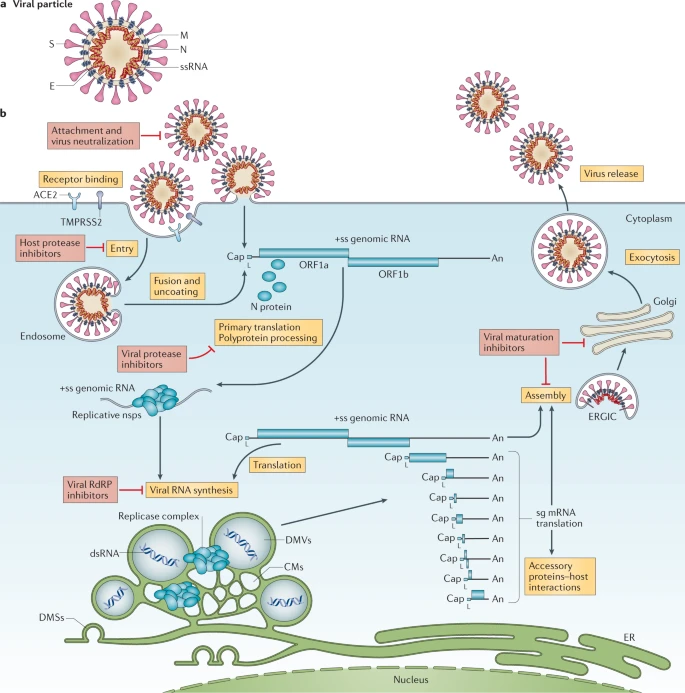
Molnupiravir is a nucleoside analog that we have discussed before but it essentially is incorporated into the growing RNA strand of a new virus by the RNA-dependent RNA polymerase which messes up the RNA & can't continue to make new virus
https://twitter.com/MonicaGandhi9/status/1415093950000422912
So, what is new drug that came out in press release today from Pfizer? PROTEASE INHIBITOR, described here. When virus enters cell, its RNA is "translated" (made into a protein) by host; that protein is very long & needs to be cut up into separate enzymes
breakthroughs.com/foundations-sc…
breakthroughs.com/foundations-sc…
to help viral replication. The protein that cuts the "polypeptide" (long protein) up is the protease so a protease inhibitor stops it. Of note, we use protease inhibitors for treatment in HIV all the time & they often come with a "booster" of their drug levels called ritonavir.
This protease inhibitor also comes co-formulated with ritonavir to boost its levels. The Pfizer protease inhibitor is called PAXLOVID as its brand name but the protease inhibitor (PI) drug is PF-07321332 and it comes with ritonavir. Press release here
pfizer.com/news/press-rel…
pfizer.com/news/press-rel…
This was phase 2/3 study called EPIC-HR (Evaluation of Protease Inhibition for COVID-19 in High-Risk Patients) -Non-hospitalized adult patients with COVID-19 all at high risk of progressing to severe illness (non-vaccinated); also studying for lower risk + household contacts
For those given inhibitor either within 3 days or 5 days after symptoms, 89% reduction in risk of COVID-19-related hospitalization or death from any cause compared to placebo: 1.0% of patients who received med within 5 days hospitalized (6/607) vs 6.7% (41/612) in placebo arm.
0 deaths in those who got PAXLOVID, 10 deaths in those who got the placebo (pill with nothing in it). So, this is a twice a day medication given for 5 days just like molnupiravir. Oral, give to someone after diagnosis & high chance of preventing severe disease in someone at risk
Also, oral antiviral medications will inhibit viral replication so less able to transmit to others (like in household where transmission highest). So, we have prevention (vaccines) and we have treatment that is oral & easy (monoclonal antibodies harder - IV or injection). Control
• • •
Missing some Tweet in this thread? You can try to
force a refresh




