
This is an extremely difficult time to be a scientist & even more so if you are a minority #WomanInScience.
Last night I went on @globalnews radio thinking I was going to talk about the differences between PCR & other screening methods for COVID—basically science.
1/
Last night I went on @globalnews radio thinking I was going to talk about the differences between PCR & other screening methods for COVID—basically science.
1/

The conversation was steered towards border policy & that some want more restrictions to be removed. Doing my duty as a scientist & using the best current evidence, I noted the rise in cases 🌍, the not so perfect💉 rate in some places & importance of using #RapidTest
2/
2/
I then urged my fellow Canadians to be prudent & cautious when making travel arrangements.
The host then made an off-the-cuff remark on how “if I were in charge of making that policy I would probably close the border”—a completely inappropriate misinterpretation of my advice‼️
3/
The host then made an off-the-cuff remark on how “if I were in charge of making that policy I would probably close the border”—a completely inappropriate misinterpretation of my advice‼️
3/
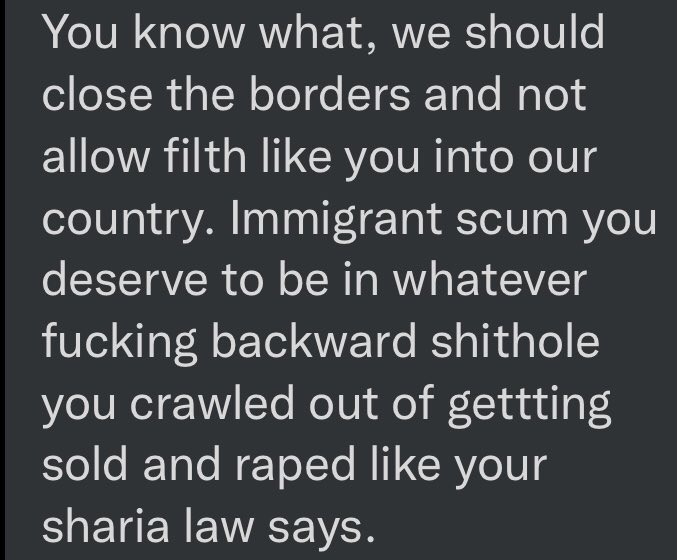
And so pour in the hate mail, calling me a “filthy immigrant” who is planning to ruin people’s holiday plans by my tyranny‼️
The proper journalistic approach would have been for the host to ask me what policy advice, if any, I’d give to those in charge of border control.
4/
The proper journalistic approach would have been for the host to ask me what policy advice, if any, I’d give to those in charge of border control.
4/
To which I would’ve said
I’m not a policy expert, I can only offer my opinion based on best current data & that we’ve a lot of tools like #RapidTests & #VaccineMandates at our disposal to help make travel safer.
I was right there but he chose to speak for me—a female scientist
5/
I’m not a policy expert, I can only offer my opinion based on best current data & that we’ve a lot of tools like #RapidTests & #VaccineMandates at our disposal to help make travel safer.
I was right there but he chose to speak for me—a female scientist
5/
I am an ex-refugee who through kindness of many Canadians was able to afford an education & transform into a scientist. I see sharing my expertise & doing media outreach as a way of paying it forward—these are on top of all other responsibilities & uncompensated‼️
6/
6/
I, like many of my peers, do what I do because I care, my only motivation & drive is to keep our communities safe‼️
Whilst the hate comes with the territory (it shouldn’t, but it does), we all play a role in tackling hate and by gods of cheesecake we CAN and MUST do better‼️
fin/
Whilst the hate comes with the territory (it shouldn’t, but it does), we all play a role in tackling hate and by gods of cheesecake we CAN and MUST do better‼️
fin/
• • •
Missing some Tweet in this thread? You can try to
force a refresh




