Treatment principles in Crohn's disease: a graphical thread 🧵 (n~28)
There is lots covered here
• impact of CD
• early effective therapy
• surgical trends
• biosimilars
• head to head studies
• mucosal healing
Follow along below👇
There is lots covered here
• impact of CD
• early effective therapy
• surgical trends
• biosimilars
• head to head studies
• mucosal healing
Follow along below👇

Crohn's disease can have a significant impact on a person's life:
• physical aspects
• psychological aspects
• long-term complications of disease (and therapy)
• everyday life
We should remember this as physicians when we talk to our patients in clinic
• physical aspects
• psychological aspects
• long-term complications of disease (and therapy)
• everyday life
We should remember this as physicians when we talk to our patients in clinic

This thread is based on a lecture I gave to the 1st annual BRICS IBD Symposium (Brazil - Russia - India - China - South Africa) last weekend
I recorded the talk which you can watch here
I recorded the talk which you can watch here
Unfortunately treatment failure and disease progression are common in Crohn's disease
• many patients have had Crohn's disease for a long time
• we have not always had effective therapies
• nor have we known to use therapies effectively until now
• many patients have had Crohn's disease for a long time
• we have not always had effective therapies
• nor have we known to use therapies effectively until now

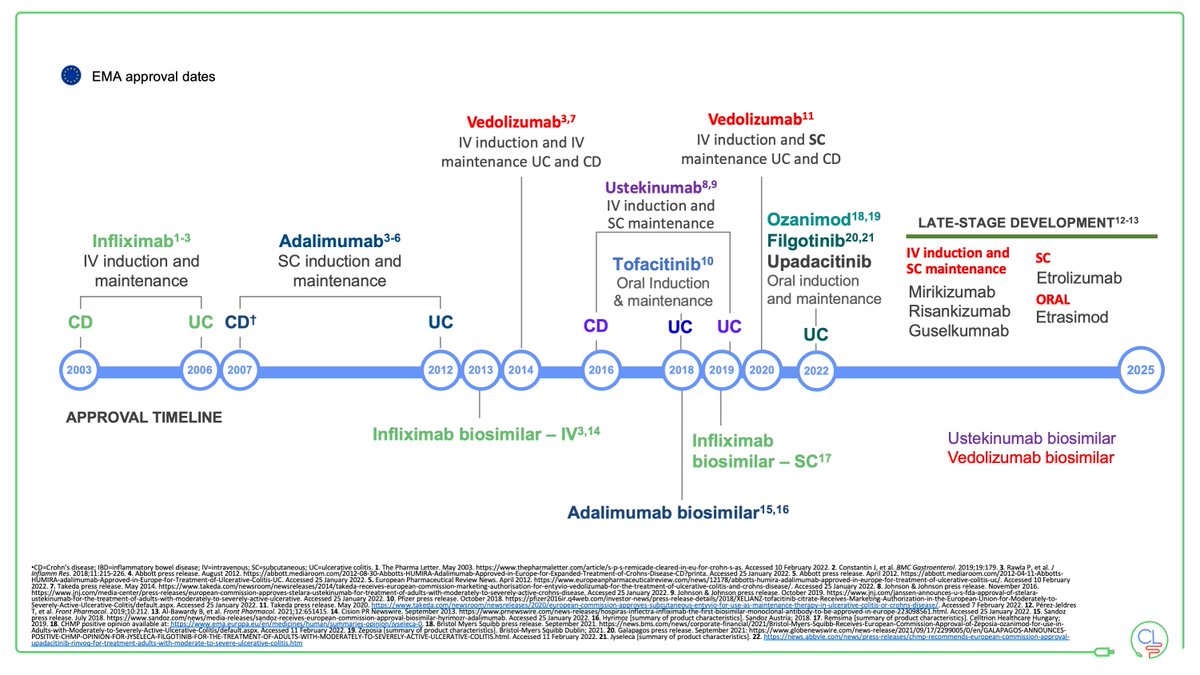
We are now in the multi-drug era for treating both Crohn's disease and UC
This is really the biosimilar anti-TNF era
This is the time when anti-TNF therapy should be affordable to all
And should not cost more than 2000 GBP per year
That changes everything
This is really the biosimilar anti-TNF era
This is the time when anti-TNF therapy should be affordable to all
And should not cost more than 2000 GBP per year
That changes everything

We know that Crohn's disease is progressive
Early in the disease course inflammation predominates
This is why early effective therapy works
The data from the anti-TNF studies shows this very clearly
Early in the disease course inflammation predominates
This is why early effective therapy works
The data from the anti-TNF studies shows this very clearly

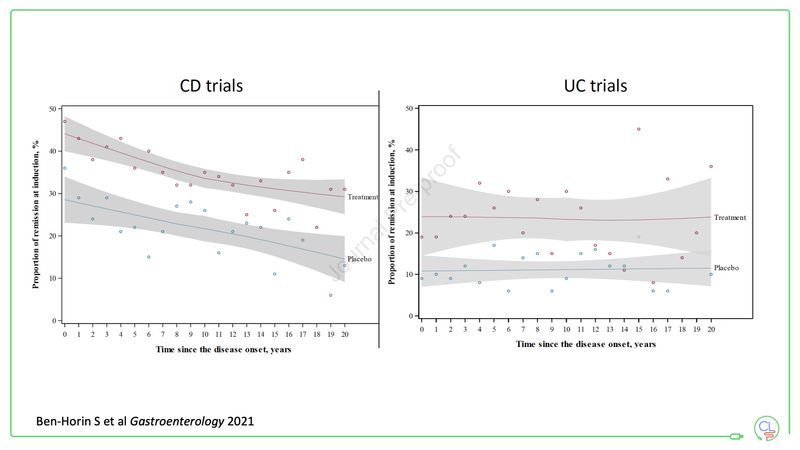
This recent brilliant analysis by @ShomronH (individual patient level meta-analysis of RCTs) clearly shows the effect:
• in Crohn's disease the biggest benefit from biologics comes with a shorter disease duration
• BUT we do not see this effect in UC
gastrojournal.org/article/S0016-…
• in Crohn's disease the biggest benefit from biologics comes with a shorter disease duration
• BUT we do not see this effect in UC
gastrojournal.org/article/S0016-…
Our data in Edinburgh by @PhilWJenkinson show the change in biologic prescribing over the last 20 years
Note how the shape of the curve changes in the right hand panel - in recent years more top down therapy
This is associated with fewer surgeries
academic.oup.com/ecco-jcc/artic…
Note how the shape of the curve changes in the right hand panel - in recent years more top down therapy
This is associated with fewer surgeries
academic.oup.com/ecco-jcc/artic…

We have been early adopters of biosimilars in the UK and especially in Edinburgh
This has facilitated big cost savings for the health service
We have re-invested this into our service
It has allowed us to use effective therapy early
And get access to newer therapies
This has facilitated big cost savings for the health service
We have re-invested this into our service
It has allowed us to use effective therapy early
And get access to newer therapies

You can see how our use of adalimumab has increased over time
This is almost all Crohn's disease (we use very little ADA in UC)
The rise in ADA prescribing anticipated the switch to biosimilar in 2018/9
@LauranneDerikx published our data academic.oup.com/ecco-jcc/advan…
This is almost all Crohn's disease (we use very little ADA in UC)
The rise in ADA prescribing anticipated the switch to biosimilar in 2018/9
@LauranneDerikx published our data academic.oup.com/ecco-jcc/advan…

This is the most important chart
• at diagnosis we need to predict risk of complicated disease
• we need to stratify therapy according to predicted response
However, we cannot yet do this ... therefore we must use a treat-to-target approach to monitor and adjust accordingly
• at diagnosis we need to predict risk of complicated disease
• we need to stratify therapy according to predicted response
However, we cannot yet do this ... therefore we must use a treat-to-target approach to monitor and adjust accordingly

Treat-to-target per STRIDE-2
The framework is simple
• set a target btwn physician & patient
• control symptoms; achieve mucosal healing; normalise QoL
• treat & monitor (CRP, FCAL + colonoscopy + MRI)
• if target not reached adjust therapy & proceed
gastrojournal.org/article/S0016-…
The framework is simple
• set a target btwn physician & patient
• control symptoms; achieve mucosal healing; normalise QoL
• treat & monitor (CRP, FCAL + colonoscopy + MRI)
• if target not reached adjust therapy & proceed
gastrojournal.org/article/S0016-…

Precision medicine may not have given us all the answers to predicting risk in Crohn's disease
But we are not completely blind
The criteria listed here have stood the test of time
E.g. always start biologics at diagnosis with fistulas & extensive disease & deep ulcers
But we are not completely blind
The criteria listed here have stood the test of time
E.g. always start biologics at diagnosis with fistulas & extensive disease & deep ulcers

How to decide who gets biologics in Crohn's disease?
Start at diagnosis (within 3m) with fistulas & extensive disease & deep ulcers & other risk factors
And start early (1st year) if FCAL does not normalise (<250mcg/g)
By @plevrisn cghjournal.org/article/S1542-…
Start at diagnosis (within 3m) with fistulas & extensive disease & deep ulcers & other risk factors
And start early (1st year) if FCAL does not normalise (<250mcg/g)
By @plevrisn cghjournal.org/article/S1542-…

In the multi-drug era of IBD we have multiple effective therapies
How then to choose the right drug for the right patient at the right time?
This is often guided by cost
• Start biosimilar anti-TNF early in those where suitable
• For those where it is not use VEDO or USTE
How then to choose the right drug for the right patient at the right time?
This is often guided by cost
• Start biosimilar anti-TNF early in those where suitable
• For those where it is not use VEDO or USTE
Anti-TNF therapy is cheap and highly effective in Crohn's disease
Safety profile is well understood
BUT there is a problem
• 20% will not respond
• many will lose response
After anti-TNF failure other drugs work less well
Safety profile is well understood
BUT there is a problem
• 20% will not respond
• many will lose response
After anti-TNF failure other drugs work less well

Head to head studies have been highly informative in IBD over the years
The misconception is that these are new - let's revisit this for Crohn's disease now
The misconception is that these are new - let's revisit this for Crohn's disease now

Remember SONIC? Published in 2010 y @JeanFredericCo1
• IFX plus AZA was best
• IFX monotherapy was next best
• AZA monotherapy was worst
We said "what if cost was no barrier?"
Well ... we now live in that world
That's why AZA monotherapy is dead
nejm.org/doi/full/10.10…
• IFX plus AZA was best
• IFX monotherapy was next best
• AZA monotherapy was worst
We said "what if cost was no barrier?"
Well ... we now live in that world
That's why AZA monotherapy is dead
nejm.org/doi/full/10.10…

Step-up versus top-down in 2008!
The study that almost got it right? The clues were all there.
Early therapy is best.
A few tweaks to the design then and we could have shown what we now know to be true. There was too much here for the detractors!
The study that almost got it right? The clues were all there.
Early therapy is best.
A few tweaks to the design then and we could have shown what we now know to be true. There was too much here for the detractors!

CALM - @JeanFredericCo1 (again) 2018
Adalimumab early in the disease course with a treat-to-target paradigm
• mucosal healing rates of 45.9% at one year
• FCAL <250mcg/g most impt driver of Rx escalation
NOW a cost-effective option
We use ADA monoRx a lot for early Crohn's
Adalimumab early in the disease course with a treat-to-target paradigm
• mucosal healing rates of 45.9% at one year
• FCAL <250mcg/g most impt driver of Rx escalation
NOW a cost-effective option
We use ADA monoRx a lot for early Crohn's

SEAVUE - another early Crohn's disease study
Both ADA and USTE work really well
Excellent clinical remission and mucosal healing rates at one year
Better safety & PK profile for USTE
Both ADA and USTE work really well
Excellent clinical remission and mucosal healing rates at one year
Better safety & PK profile for USTE

Importantly now we have many drugs that will heal the mucosa in Crohn's disease: IFX, ADA, USTE and VEDO of the licensed therapies
Most widespread definition is absence of ulcers
Mucosal healing remains THE treatment target in Crohn's disease
Most widespread definition is absence of ulcers
Mucosal healing remains THE treatment target in Crohn's disease

Anti-TNF drugs have been shown multiple times to be superb drugs to achieve mucosal healing
Nothing else could do this before they came along
We've had them >20 years now - only just starting to use them effectively!
Nothing else could do this before they came along
We've had them >20 years now - only just starting to use them effectively!

USTE will heal the mucosa in Crohn's disease
The data from SEAVUE really add to this
The data from SEAVUE really add to this

VEDO also heals the mucosa in Crohn's disease
The data from VERSIFY (pictured) and CD-LOVE and VISIBLE 2 show this
The data from VERSIFY (pictured) and CD-LOVE and VISIBLE 2 show this

The data on new molecules look very exciting too
The RIZA induction data show that mucosal healing is achieved by a significant proportion after induction only
The maintenance endoscopic data are even better
The drug works when anti-TNF have failed too - this is important
The RIZA induction data show that mucosal healing is achieved by a significant proportion after induction only
The maintenance endoscopic data are even better
The drug works when anti-TNF have failed too - this is important

Soon we will also talk about effective dietary and microbiome therapeutics for Crohn's disease
I suspect for many these will be adjuncts to effective medical therapies
But for some they may be sufficient by themselves
We need much more quality research here
I suspect for many these will be adjuncts to effective medical therapies
But for some they may be sufficient by themselves
We need much more quality research here

These slides are the basis of my talk on Crohn's disease: treatment principles and mucosal healing
It is recorded and uploaded here for you to watch:
It is recorded and uploaded here for you to watch:

Our team are working hard to produce many of these data
We are showing the benefit of
• biosimilars in IBD
• early effective therapy in Crohn's disease
• advance therapies in UC
• reduced surgical rates
• optimal use of T2T strategies based on FCAL
Lots more to come ..
We are showing the benefit of
• biosimilars in IBD
• early effective therapy in Crohn's disease
• advance therapies in UC
• reduced surgical rates
• optimal use of T2T strategies based on FCAL
Lots more to come ..

Please leave comments below and go back to the top and share the first tweet ... this allows other to learn from the whole thread
https://twitter.com/charlie_lees/status/1463628917022076938?s=20
The low down on Crohn's disease therapy:
• early effective therapy is key
• FCAL in year 1 is an excellent marker
• biosimilars make anti-TNF therapy an excellent option
• USTE & VEDO also good options for mucosal healing
• new therapies (esp anti-p19 eg RIZA) look superb
• early effective therapy is key
• FCAL in year 1 is an excellent marker
• biosimilars make anti-TNF therapy an excellent option
• USTE & VEDO also good options for mucosal healing
• new therapies (esp anti-p19 eg RIZA) look superb
• • •
Missing some Tweet in this thread? You can try to
force a refresh