
THREAD on the new variant B.1.1.529 summarising what is known from the excellent South African Ministry of Health meeting earlier today
TLDR: So much uncertain but what *is* known is extremely worrying & (in my opinion) we should revise red list immediately.
This is why: 1/16
TLDR: So much uncertain but what *is* known is extremely worrying & (in my opinion) we should revise red list immediately.
This is why: 1/16
The South African Ministry of Health had a live streamed briefing today on the new variant detected there.
The variant was identified this week and has been found in three countries so far: Botswana, South Africa and Hong Kong (returning traveller). 2/16
The variant was identified this week and has been found in three countries so far: Botswana, South Africa and Hong Kong (returning traveller). 2/16
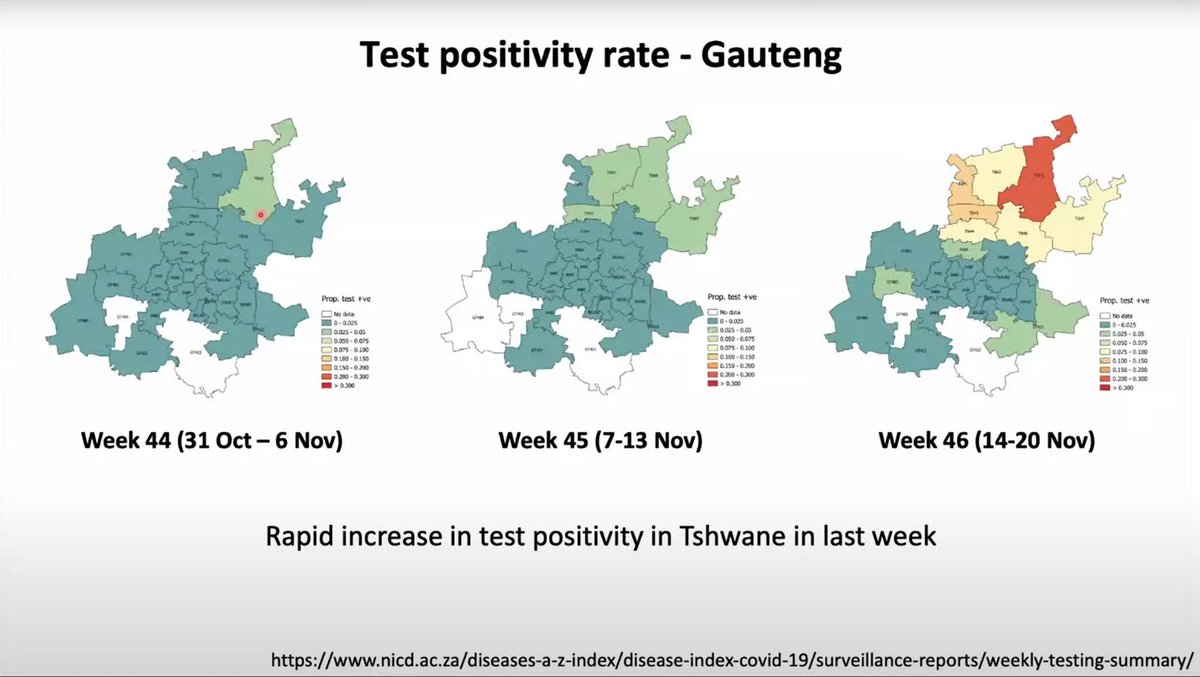
In South Africa it has been detected in Guateng province - positivity rates in Tshwane (part of Guateng) have increased massively in the last 3 weeks from less than 1% to over 30%.
3/16
3/16
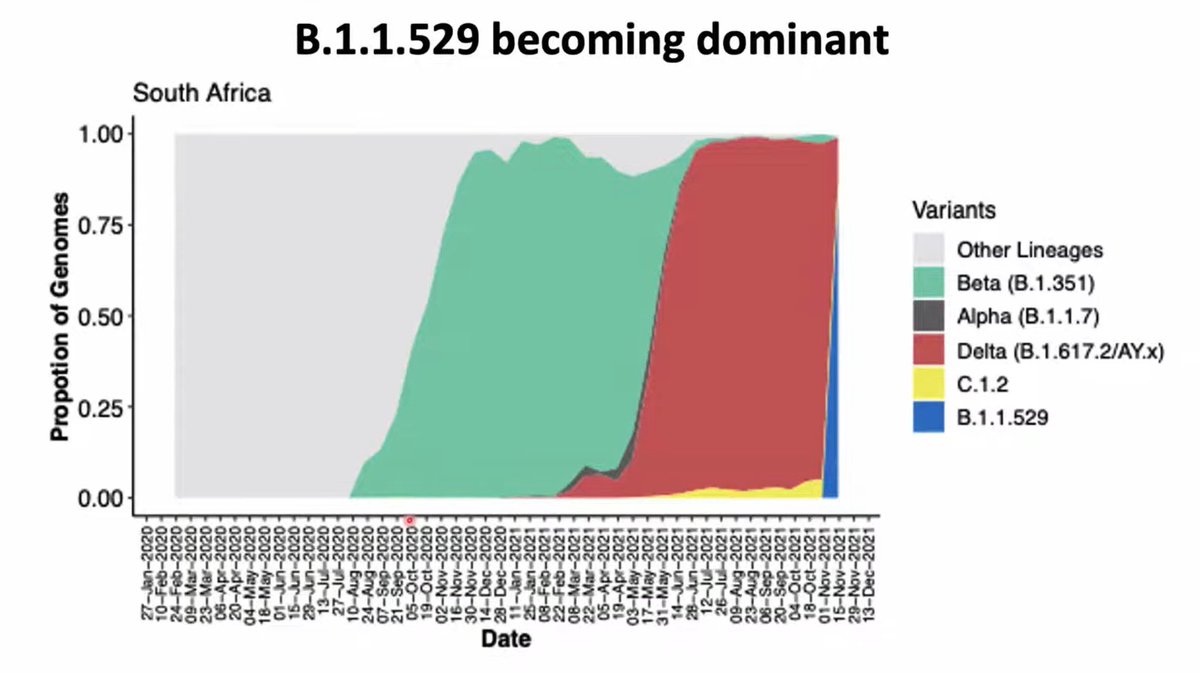
Because of this increase, COVID sequencing has been concentrated on samples from Guateng.
Almost all recent samples from there (77) have been this new variant (blue dots) - taking over from a background of Delta (red) and C.1.2 (also a concerning variant, yellow). 4/16
Almost all recent samples from there (77) have been this new variant (blue dots) - taking over from a background of Delta (red) and C.1.2 (also a concerning variant, yellow). 4/16

SA had a big Delta surge over June and July but recent rates were very very low. Most recent days have seen early surge, mainly driven by Guateng.
SA has high levels of prev infection from 3 very large waves but relatively low levels of vaccination (~24% fully vaxxed). 5/16
SA has high levels of prev infection from 3 very large waves but relatively low levels of vaccination (~24% fully vaxxed). 5/16

The bias of sequences towards Guateng means that it looks as if B.1.1.529 is rapidly taking over from Delta (red) and C.1.2 (yellow) on chart of sequenced cases - but few samples.
BUT there is one stroke of luck - it also has "S-gene dropout" like Alpha did, which means... 6/16
BUT there is one stroke of luck - it also has "S-gene dropout" like Alpha did, which means... 6/16
...that we can track it across all PCR positive cases that used a specific type of test (TaqPath). This means much better real time data.
BUT that's where the good news stops - because S-gene drop out data suggests it's rapidly increasing across S Africa. 7/16
BUT that's where the good news stops - because S-gene drop out data suggests it's rapidly increasing across S Africa. 7/16

And in a regional breakdown, you see the same vertical spike in almost all regions. This + traveller from SA case in Hong Kong suggests B.1.1.529 already widespread in SA and that other regions might follow Guateng's rise soon. 8/16

The sheer increase on these charts is very worrying and suggests that B.1.1.529 might have significant advantages over Delta and C.1.2. What exactly this advantage is and how it breaks down between immune escape and transmissibility is not yet known.
BUT 9/16
BUT 9/16
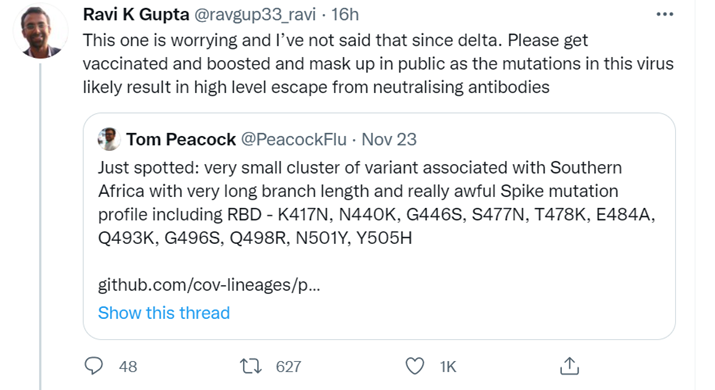
We do know that B.1.529 has many more mutations than other variants *and* has mutations seen in other variants that are associated with BOTH higher transmissibility AND immune escape.
It's the number and type of mutations that are worrying the virologists & immunologists 10/16
It's the number and type of mutations that are worrying the virologists & immunologists 10/16

The SA science establishment & Ministry of Health transparency are doing *a global service* - we *cannot* underestimate how important their work and transparency are this week.
They are urgently doing lab experiments to understand it more & continuing to track spread 11/16
They are urgently doing lab experiments to understand it more & continuing to track spread 11/16
A new UKHSA technical briefing on variants is due tomorrow - I am sure they will at least mention this variant. WHO are meeting about it today as well.
People working in this field in England at the highest levels are very concerned 12/16
People working in this field in England at the highest levels are very concerned 12/16
Given the speed with which this variant has spread & mutations which *might* mean signifcant vaccine escape, in my opinion the UK should get ahead of this *right now*.
As far as we know, it's not here yet.
*Adding SA and close neighbours to the red list seems sensible* 13/16
As far as we know, it's not here yet.
*Adding SA and close neighbours to the red list seems sensible* 13/16
Because of UK status as international travel hub, v few restrictions in UK and the worrying signs from SA, we must act now or risk it being too late.
Regardless of travel restrictions, supporting S African response as Barrett suggests is the right thing to do. 14/16
Regardless of travel restrictions, supporting S African response as Barrett suggests is the right thing to do. 14/16

If it's a false alarm, then we can step down response in a few weeks. But this is our window to act. As with Delta (and B.1.1.529 seems to spreading as or more quickly), waiting for certainty risks waiting too long.
15/16
15/16
Finally, this is just my opinion.
It's hopefully not here yet. We don't have definitive evidence on transmission advantage or immune escape but we have plenty of cause to suspect both.
Let's be super protective of our vaccine programme and take precautionary action. 16/16
It's hopefully not here yet. We don't have definitive evidence on transmission advantage or immune escape but we have plenty of cause to suspect both.
Let's be super protective of our vaccine programme and take precautionary action. 16/16
NB they reported a big backlog yesterday so recent increase artificially big! I don't think it affects the other charts though which are directly from the ministry presentation
• • •
Missing some Tweet in this thread? You can try to
force a refresh






















