
Why did observational studies find ⬆️survival for late dialysis initiation, whereas the IDEAL RCT found no difference? Was it confounding, the usual culprit we point to? No!
Our new paper @bmj_latest addresses this and much more! #epitwitter #nephtwitter
bmj.com/content/375/bm…
Our new paper @bmj_latest addresses this and much more! #epitwitter #nephtwitter
bmj.com/content/375/bm…
By carefully reading the previous observational studies (refs 14-32 in our paper), we identified that virtually all of them suffered from study design errors
This introduced 3 preventable biases, ON TOP OF confounding
1⃣ lead time bias
2⃣ immortal time bias
3⃣ survivor bias
2/n
This introduced 3 preventable biases, ON TOP OF confounding
1⃣ lead time bias
2⃣ immortal time bias
3⃣ survivor bias
2/n
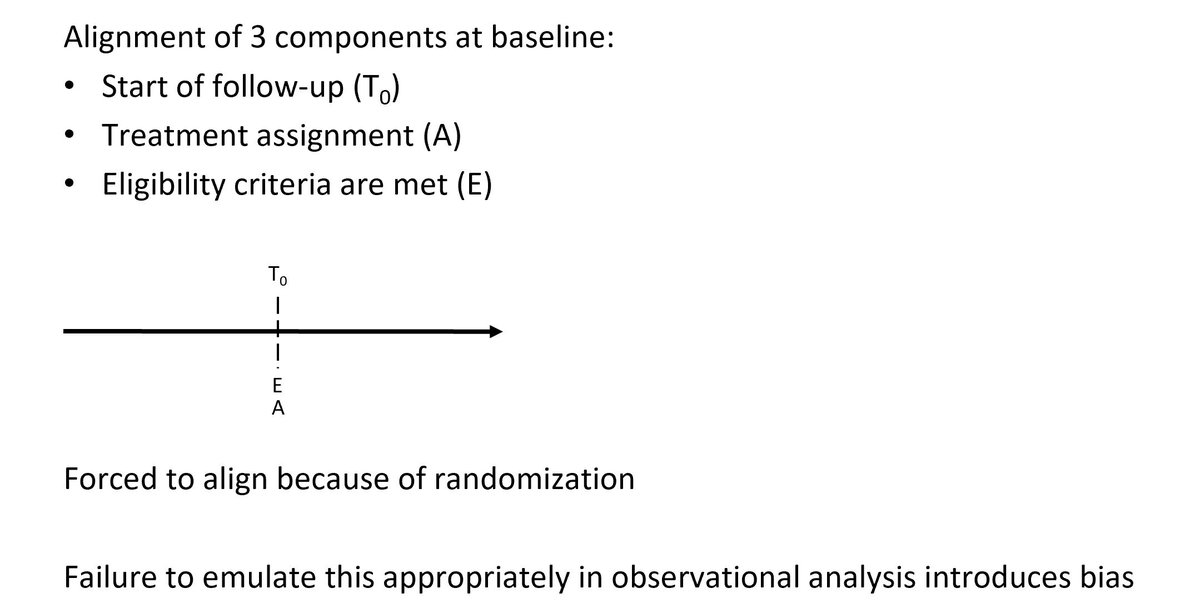
These 3 biases occur if investigators do not emulate the strict design criteria of a clinical trial
In a trial, start of follow-up & assignment of treatment strategies align
If you do not do align these in your observational study, you introduce bias 3/n
pubmed.ncbi.nlm.nih.gov/27237061/
In a trial, start of follow-up & assignment of treatment strategies align
If you do not do align these in your observational study, you introduce bias 3/n
pubmed.ncbi.nlm.nih.gov/27237061/
In an RCT, we'd randomize pts with eGFR of 10-20 ml/min to start early (eGFR 10-14) or late (eGFR 5-7). Follow-up thus starts at randomization, which is when the treatment is ASSIGNED, but NOT necessarily STARTED (dialysis is started in the future, but only if pt survives) 4/n
... Thus, treatment assignment & start of follow-up align
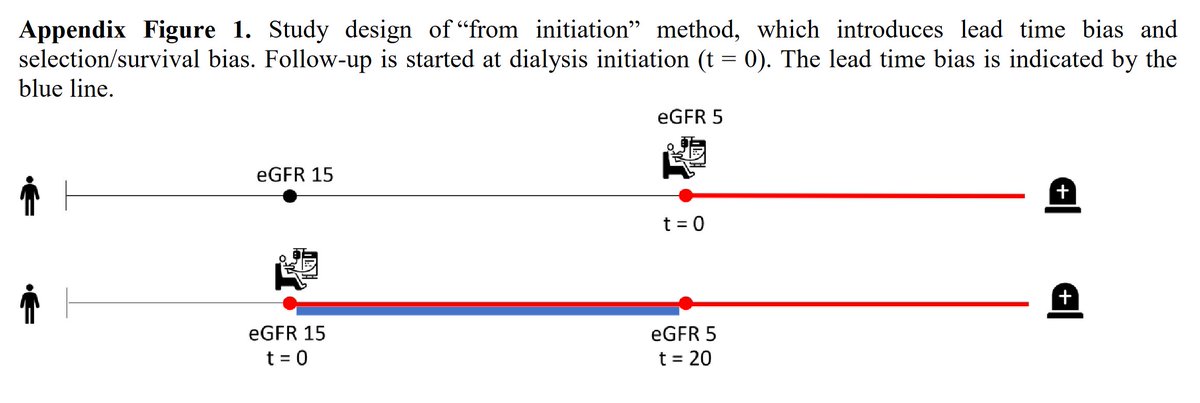
However, many observational studies started their follow-up at dialysis initiation, which would not be possible in an RCT❗️ This introduces lead time bias & survivor bias. 5/n
However, many observational studies started their follow-up at dialysis initiation, which would not be possible in an RCT❗️ This introduces lead time bias & survivor bias. 5/n
Lead time bias b/c patients with higher eGFR are followed from an earlier point in time (in fig below, lead time is indicated w/ blue line)
This gives artificial survival advantage to EARLY starters. However, observ studies found survival benefit for LATE starters ⁉️
6/n
This gives artificial survival advantage to EARLY starters. However, observ studies found survival benefit for LATE starters ⁉️
6/n
B/c there is another bias: Survivor bias! Pts surviving until low eGFR MUST have less risk factors for☠️ than pts who start early. Only strong survivors remain in late start group b/c people with low eGFR AND many risk factors will die before they can start dialysis late...
7/n
7/n
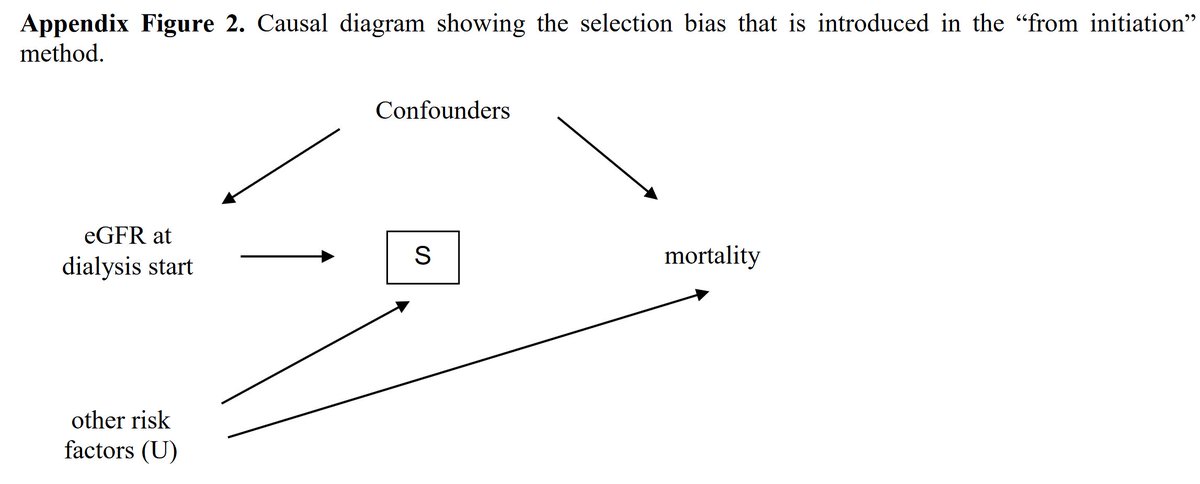
In the epi literature we call this "collider stratification bias". This is distinct from confounding.
It arises because we restrict our analyses to survivors ("S" in fig below). In the causal diagram below the diff between confounding and collider bias is illustrated
8/n
It arises because we restrict our analyses to survivors ("S" in fig below). In the causal diagram below the diff between confounding and collider bias is illustrated
8/n
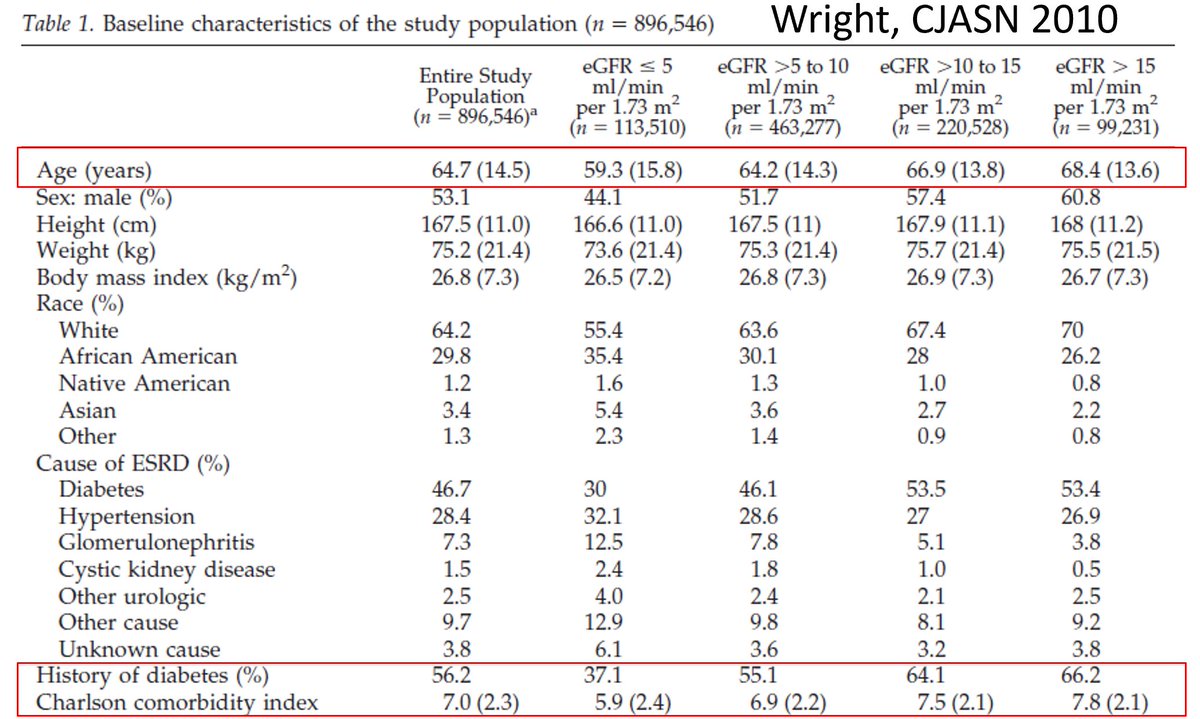
You can actually see this collider bias happening. Here is a baseline table of a previous observ study: pts starting dialysis with LOW eGFR are YOUNGER and have LESS comorbidities than pts starting at high eGFR
Very odd! You'd expect people with lower eGFR to be older ❗️
9/n
Very odd! You'd expect people with lower eGFR to be older ❗️
9/n
Other obs studies started follow-up at 1 point in time, e.g. eGFR of 20, to mitigate lead time bias. When people have not started dialysis yet at baseline, what is their Tx group?
Researchers have used future info to classify pts into groups, introducing immortal time bias
10/n
Researchers have used future info to classify pts into groups, introducing immortal time bias
10/n
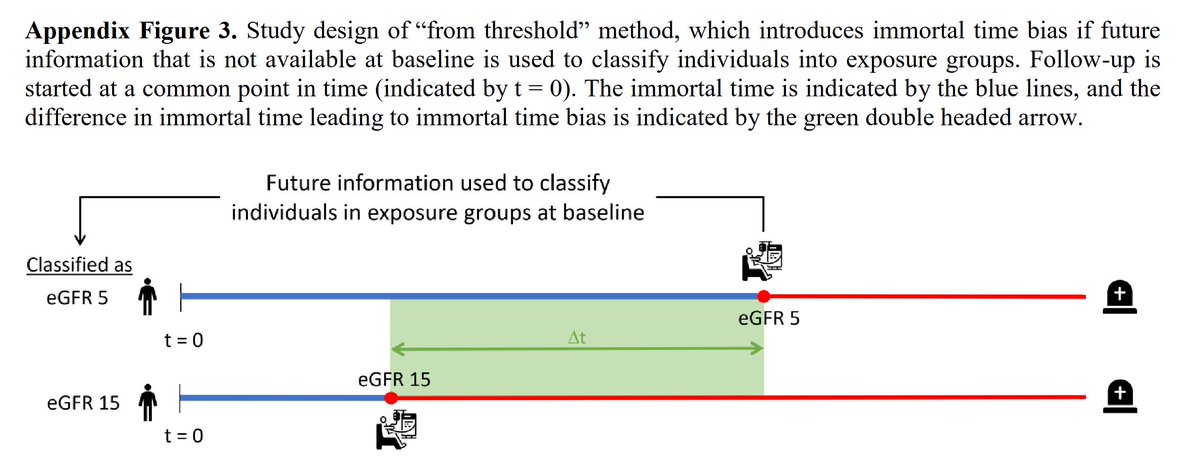
Again, in an RCT we would do this differently: we randomize individuals to different strategies at baseline, and their Tx group does not depend on whether they actually start dialysis (and at which eGFR) or not
11/n
11/n
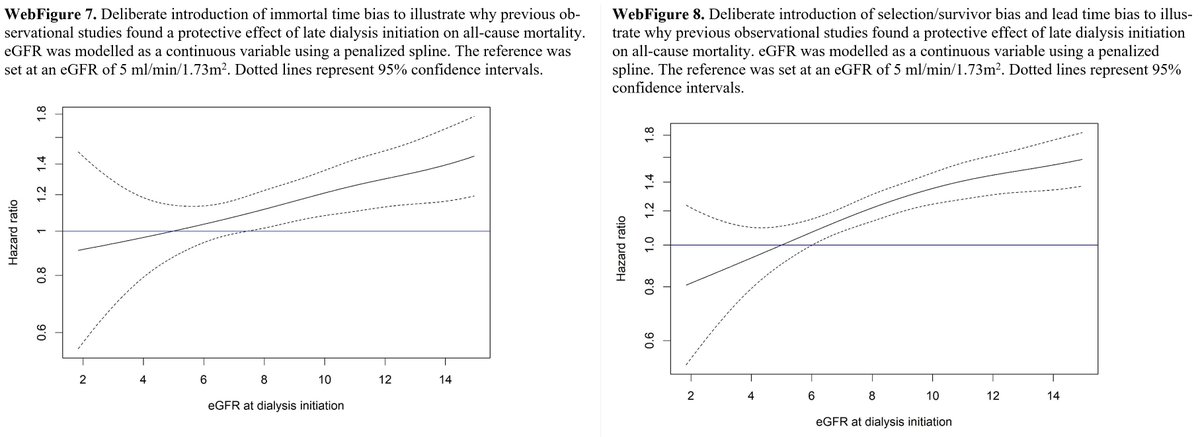
When we used the same biased study designs as prev obs studies, we actually got the same biased results: a strong survival benefit for late dialysis initiation
(remember again that the RCT found no difference)
12/n
(remember again that the RCT found no difference)
12/n
Luckily, all 3 biases are self-inflicted: they can be prevented by aligning start of FU & Tx assignment
This does require methods that were only developed in the past decade by @_MiguelHernan: target trial emulation and cloning/censoring/weighting🎯
13/n
This does require methods that were only developed in the past decade by @_MiguelHernan: target trial emulation and cloning/censoring/weighting🎯
13/n
When we explicitly emulated the strict design criteria of the IDEAL trial, and investigated the same treatment strategies, we actually found no difference between early and late dialysis: IDEAL HR 1.04 vs. our observational emulation HR 0.97 ✅
14/n
14/n
This shows that confounding was not the reason for the discrepancy between obs studies and RCTs, but rather self-inflicted biases introduced by the investigators
15/n
15/n
After benchmarking our analytical methods, we then went on to use our big dataset to go further than the IDEAL RCT:
IDEAL only investigated 2 strategies, which were only 2.2 ml/min apart. We cannot infer from 2 strategies an ideal eGFR level...
16/n
nejm.org/doi/full/10.10…
IDEAL only investigated 2 strategies, which were only 2.2 ml/min apart. We cannot infer from 2 strategies an ideal eGFR level...
16/n
nejm.org/doi/full/10.10…
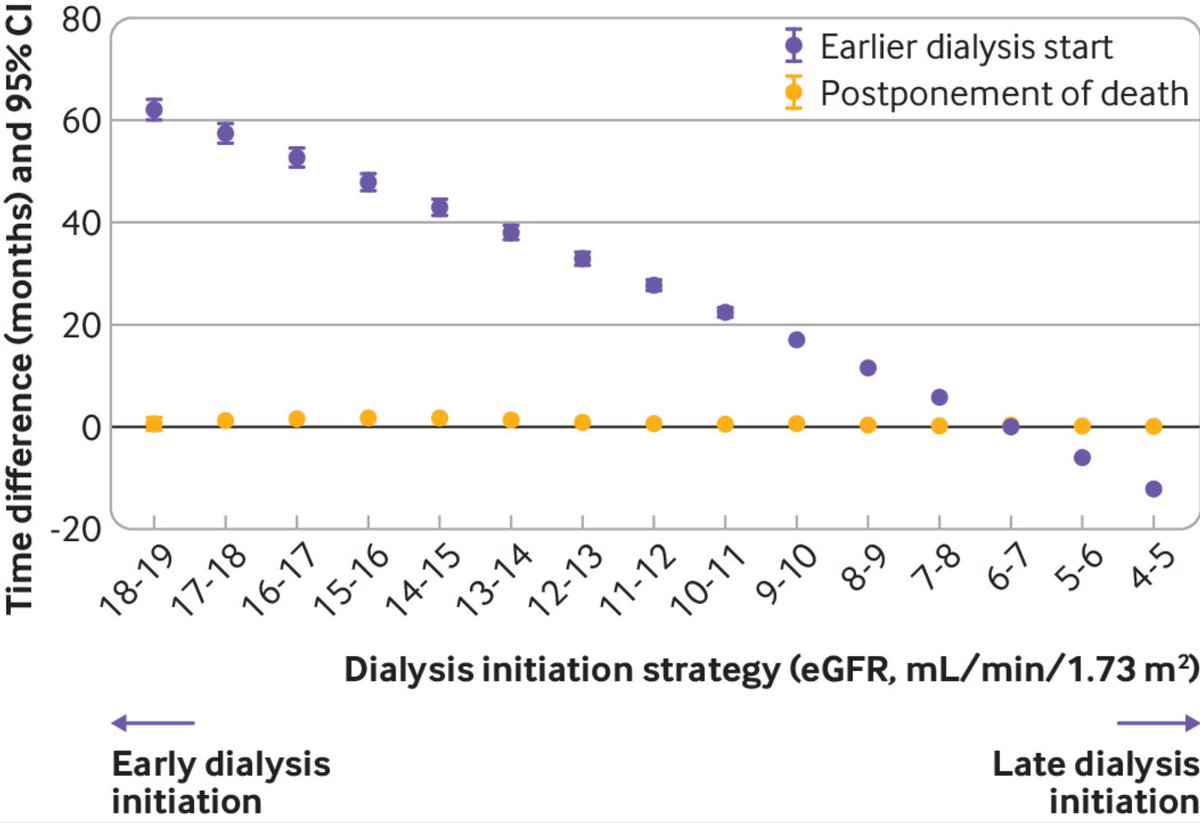
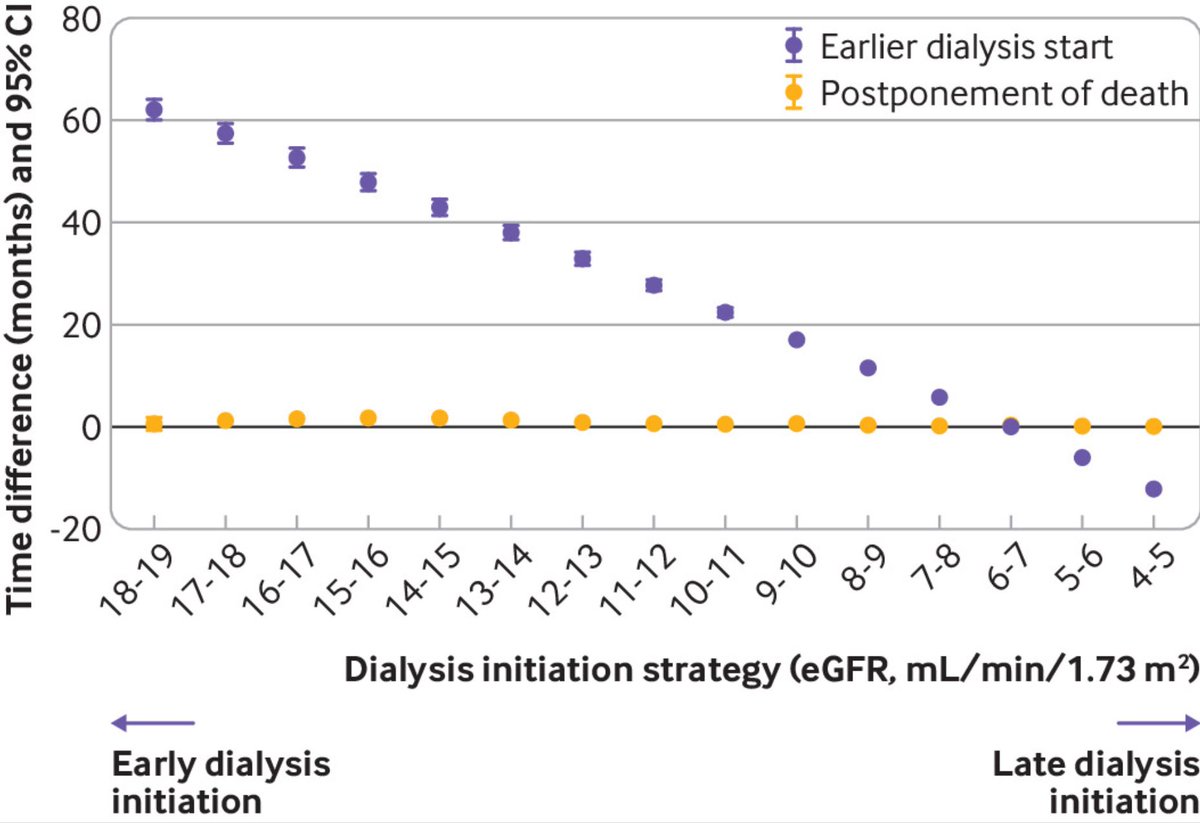
So we compared 15 different dialysis initiation strategies, of eGFR levels betw 4-19 ml/min in steps of 1 ml/min
Using the same target trial emulation methods🎯we found a small survival benefit for very early dialysis initiation: 1.6 month longer survival over 5 yrs of FU
17/n
Using the same target trial emulation methods🎯we found a small survival benefit for very early dialysis initiation: 1.6 month longer survival over 5 yrs of FU
17/n
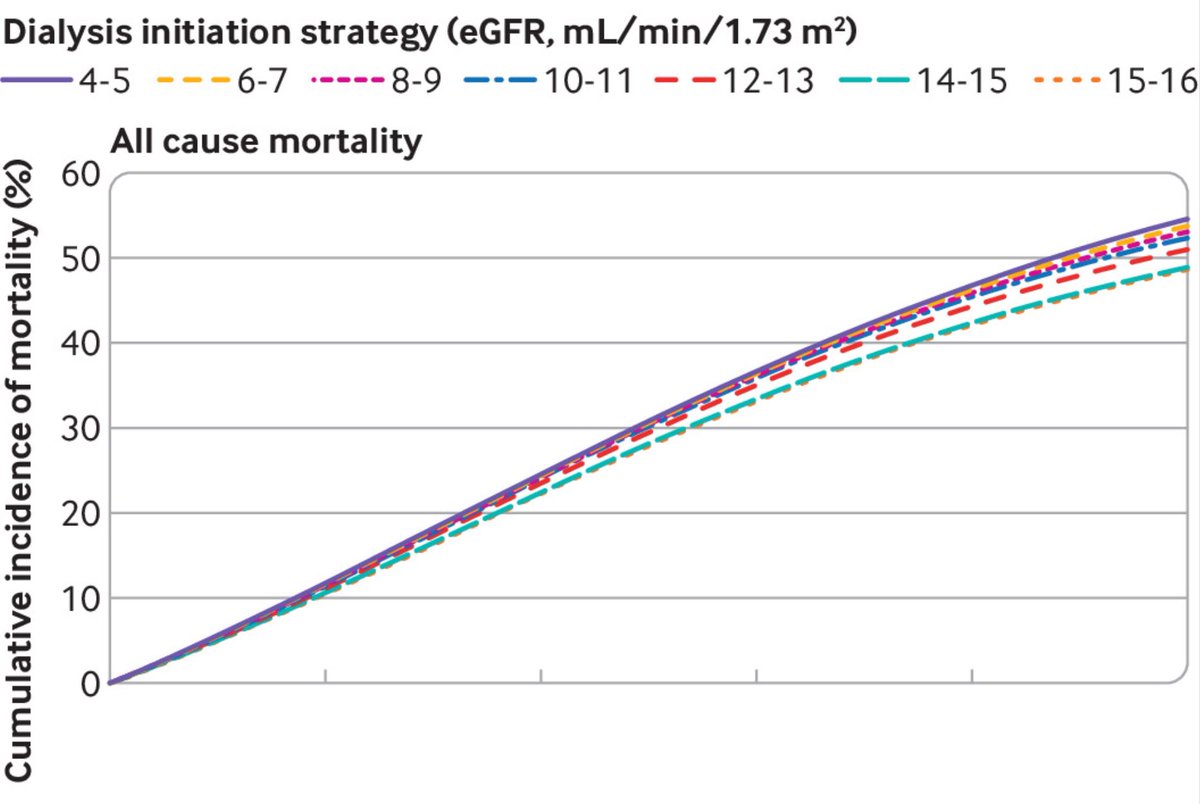
However, there is a trade-off: dialysis would need to be initiated on average 4 years earlier. For most patients, the small survival benefit may not outweigh the burden of a substantially longer period spent on dialysis.
18/n
18/n
Our study shows the value of carefully conducted observ studies. It is not RCTs vs. observ studies, but RCTs ➕observ studies - together they BOTH can provide valuable evidence for decision making
Many thanks to all coauthors and 6 reviewers (!) for invaluable comments
END 19/19
Many thanks to all coauthors and 6 reviewers (!) for invaluable comments
END 19/19
• • •
Missing some Tweet in this thread? You can try to
force a refresh


