1/ 🧵Ready to play a game #EmoryNCCTweetorials #Neurotwitter #FOAMncc ?
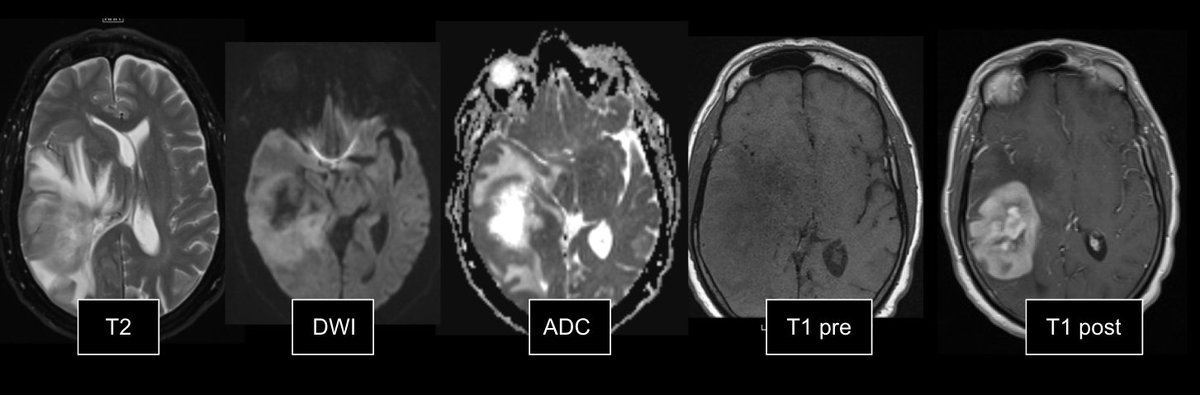
Review these images carefully. Poll in next tweet.
Review these images carefully. Poll in next tweet.

2/ What do all of these diverse #braininjury cases have in common?
3/ All of these patients developed paroxysmal sympathetic hyperactivity (PSH) or #neurostorming
Here you will find PSH resources to
✅Understand the pathophys of #PSH
✅Rule out mimics
✅Diagnose PSH
✅Treat PSH
Here you will find PSH resources to
✅Understand the pathophys of #PSH
✅Rule out mimics
✅Diagnose PSH
✅Treat PSH
4/ One accepted theory regarding the pathophysiologic basis of PSH is the "excitatory:inhibitory ratio model"
➡️pubmed.ncbi.nlm.nih.gov/28816118/
➡️pubmed.ncbi.nlm.nih.gov/28816118/
5/ Normally:
🧠multiple circuits (both cortical and subcortical) regulate activity in brainstem nuclei
🧠these circuits provide inhibition to spinal-reflex arcs that provide balance of interneuons of motor and sympathetic efferent pathways
🧠multiple circuits (both cortical and subcortical) regulate activity in brainstem nuclei
🧠these circuits provide inhibition to spinal-reflex arcs that provide balance of interneuons of motor and sympathetic efferent pathways
6/ Injury and disconnection of these inhibitory pathways lead to⬆️motor and sympathetic activity to typically non-noxious stimuli

7/ A common misconception: PSH occurs only in TBI patients
💡majority of all patients with PSH have underlying TBI
💡other brain injuries like hypoxic ischemic injury, ischemic and hemorrhagic stroke, hydrocephalus and demyelinating disease are associated with PSH
💡majority of all patients with PSH have underlying TBI
💡other brain injuries like hypoxic ischemic injury, ischemic and hemorrhagic stroke, hydrocephalus and demyelinating disease are associated with PSH
8/ We know via neuro-imaging studies that the following lesion locations are assoc. w/ PSH
🧠Diffuse axonal injury
🧠Periventricular white matter
🧠Corpus callosum
🧠Diencephalon
🧠Midbrain
🧠Pons
🧠Diffuse axonal injury
🧠Periventricular white matter
🧠Corpus callosum
🧠Diencephalon
🧠Midbrain
🧠Pons
9/ 🚨PSH is a problem
↑ICU LOS
↑Hosp LOS
↑Time on ventilator
Associated with worse outcomes in some studies
↑ICU LOS
↑Hosp LOS
↑Time on ventilator
Associated with worse outcomes in some studies
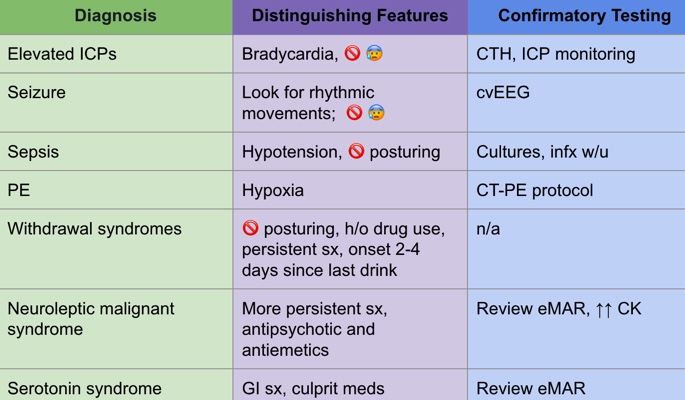
10/ So, how do you know if your patient has PSH?
1⃣They have associated brain injury (TBI, anoxic, stroke, etc.)
2⃣Use this table to help you
1⃣They have associated brain injury (TBI, anoxic, stroke, etc.)
2⃣Use this table to help you

11/ PSH is a diagnosis of exclusion. 🛑Before you diagnose PSH, look for mimics 🕵️♀️
12/ There’s a great PSH Assessment tool which can be used to aid your diagnosis
pubmed.ncbi.nlm.nih.gov/24731076/
Let’s break it down.
pubmed.ncbi.nlm.nih.gov/24731076/
Let’s break it down.
13/ First, add up all the points using the "clinical features scale"

14/ Then, add up all the points for the diagnostic likelihood tool

15/ add the 2 tools together to assess the likelihood of your diagnosis

16/ Now, it’s time to treat PSH. Make sure you have options to
🚨Abort acute episodes
🚨Start maintenance treatment if you’ve had >4 episodes or these are lasting more than 48 hours or so
🚨Abort acute episodes
🚨Start maintenance treatment if you’ve had >4 episodes or these are lasting more than 48 hours or so

17/ Don’t forget to treat/assess for urinary retention, constipation and other causes of discomfort (pain, new infections) as these can trigger PSH!
18/ What have we learned re PSH?
✅Caused by injury to inhib sympathetic and motor pathways
✅Can present ~24 hrs-weeks out from injury
✅Diagnosis of excl
✅Use scoring tool to help diagnosis
✅There are many tx options
✅Caused by injury to inhib sympathetic and motor pathways
✅Can present ~24 hrs-weeks out from injury
✅Diagnosis of excl
✅Use scoring tool to help diagnosis
✅There are many tx options
19/ Enjoy (or don't) this quick reference PSH sheet

20/ Other PSH pearls🦪 to share?
@caseyalbin @Capt_Ammonia @Tracey1milligan
@JimSiegler @AaronLBerkowitz
@drdangayach @pouyeah
@subinmatthews @JimmySuhMD @emcrit
@LDCritCare @Emcrit @EricLawson90
@neuro_intensive @caseyhall @CajalButterfly
@caseyalbin @Capt_Ammonia @Tracey1milligan
@JimSiegler @AaronLBerkowitz
@drdangayach @pouyeah
@subinmatthews @JimmySuhMD @emcrit
@LDCritCare @Emcrit @EricLawson90
@neuro_intensive @caseyhall @CajalButterfly
• • •
Missing some Tweet in this thread? You can try to
force a refresh