Here's your AB COVID # analysis for Wed Dec 29th. I'll focus on the last 24 hours, and throw in a whole bunch of caveats, because some of this data is not as useful as it used to be. 1/
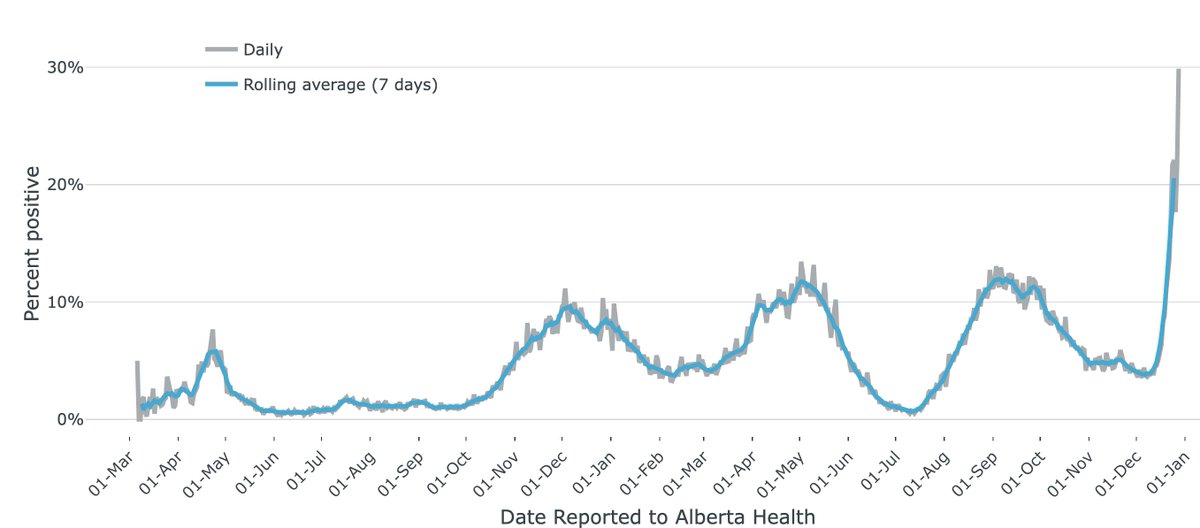
Cases/d yest 2800, a new pandemic record, and a % incr over last Tues's 1359. Except this data point is nowhere close as useful to a similar cases/d at any previous time of the pandemic, as evidenced by the record positivity of 29.88% (last Tues 11.89%). 2/ 



Hospitalizations: inpts.From a low of 261 on Sat, up +5 to 266 on Sun, +14 to 280 on Mon, and +12 to 292 yest. Not sure how useful this is, b/c it is unclear if all these new admits are pts admitted because of covid, or other reasons and just testing +ve incidentally. 3/

ICU: 57 xmas day, 57 boxing day, 60 Mon, 57 yest. This is a better data point to watch, b/c much less likely for a pt to "incidentally" catch covid in the ICU (although not impossible). 8 new paeds admits. see table from @ArynToombs for details. 4/

Deaths 11. Including 2 under the age of 50, one under the age of 40. Deaths are the other important data point to watch. Impossible to misunderstand that one. 5/

Demographics: skyrocketing cases in the 20-59 age groups. relatively sheltered are the 60-79 and 80+ age groups, protecting the most vulnerable. Let's hope this holds. And it remains very much an urban wave (so far). 6/



Feeling pretty down about the inevitability of this wave. I'm committed to doing my best to not get it... wearing a respirator when indoors, avoiding avoidable engagements, and the like. Avoiding longCOVID is my end goal. 7/
I'll end with this tweet thread I wrote this am about schools. I guess tomorrow we find out. fin/
https://twitter.com/jvipondmd/status/1476243342748909569?s=20
Thanks to @ByMatthewBlack @ArynToombs and AB Health for the graphics.
• • •
Missing some Tweet in this thread? You can try to
force a refresh