Why we #pocus: unexpected complications and daily changes. A thread.
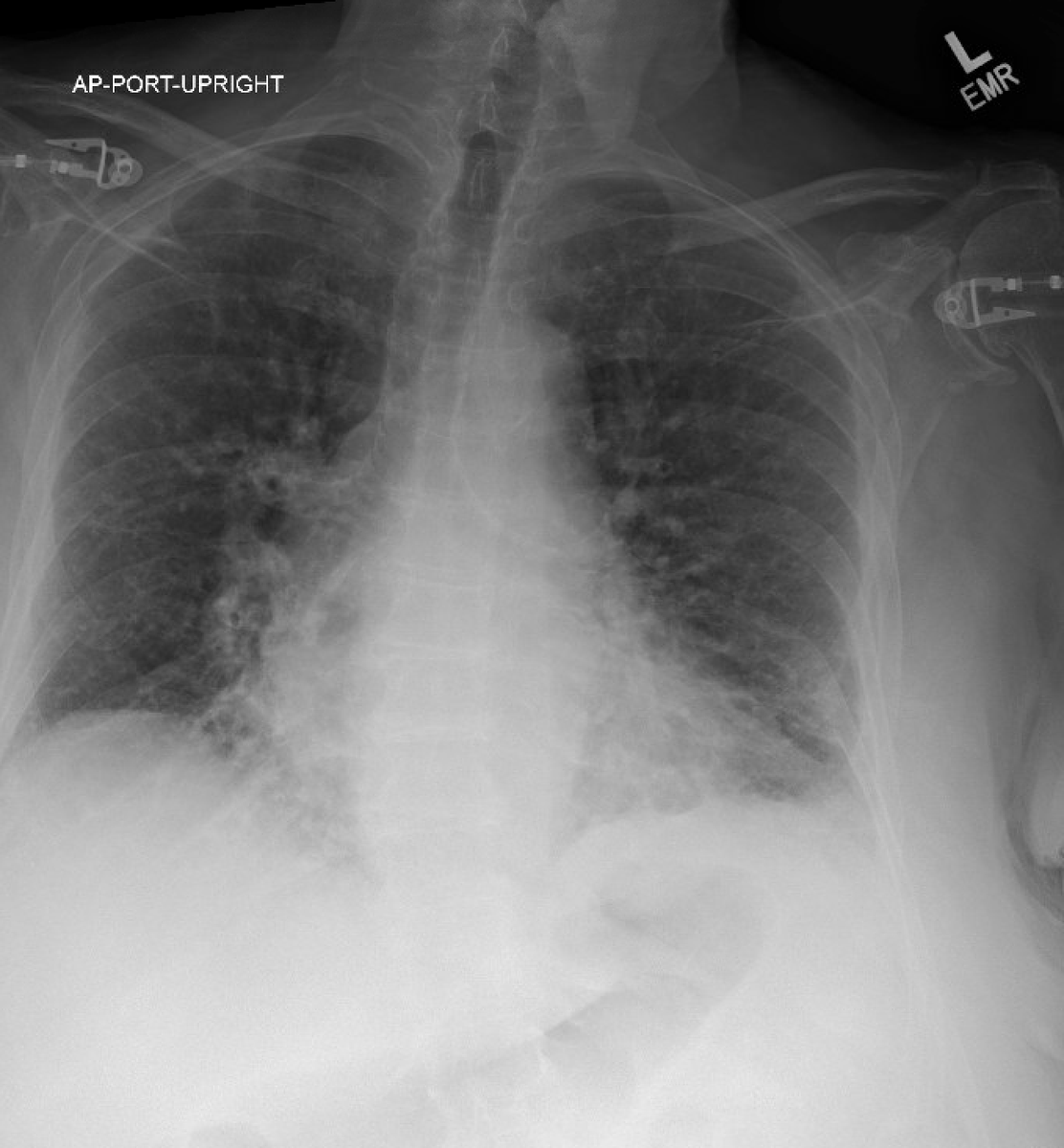
70 year old male presented with hypoxic respiratory failure. Initially diagnosed with bilateral pneumonia and started on zosyn. Very hypoxic requiring 15L. The following morning #pocus revealed:
70 year old male presented with hypoxic respiratory failure. Initially diagnosed with bilateral pneumonia and started on zosyn. Very hypoxic requiring 15L. The following morning #pocus revealed:
Large bilateral pleural effusion a with compression atelectasis. Clinically was never pneumonia. Was upgraded to ICU and intubated. R sided thoracentesis drained 1.8L of fluid and was stepped out of ICU
The following morning lung #pocus exam done. Left lung: lung sliding with diffuse lung rockets consistent with pulmonary edema
Left lung M-Mode: Sandy Beach sign consistent with normal lung sliding 

R lung anterior: A lines present but NO lung sliding
M- mode of R lung: barcode sign consistent with pneumothorax.

Couldn't find lung point so got CT to confirm:
This was a clear and excellent example of how #pocus helps patients and saves them from complications. This patient had other reasons to be hypoxic so pneumothorax was not on the differential initially. But post thoracentesis this is always a concern.
@Wilkinsonjonny @iceman_ex @NephroP @nickmmark @nilamjsoni @DRsonosRD @TaotePOCUS @POCUS_Society @POCUSAcademy @POCUS_Manifesto
A lot more about lichtenstein and his early pneumothorax studies in our book the @POCUS_Manifesto on Amazon! amazon.com/POCUS-Manifest…
• • •
Missing some Tweet in this thread? You can try to
force a refresh