#JanuAIRWAY Day 14. One Lung Ventilation – one of @vapourologist’s favourite procedures in anaesthesia – physiology in action! Here’s a #OnePager. Let’s dive in…
#JanuAIRWAY 1/9
#JanuAIRWAY 1/9

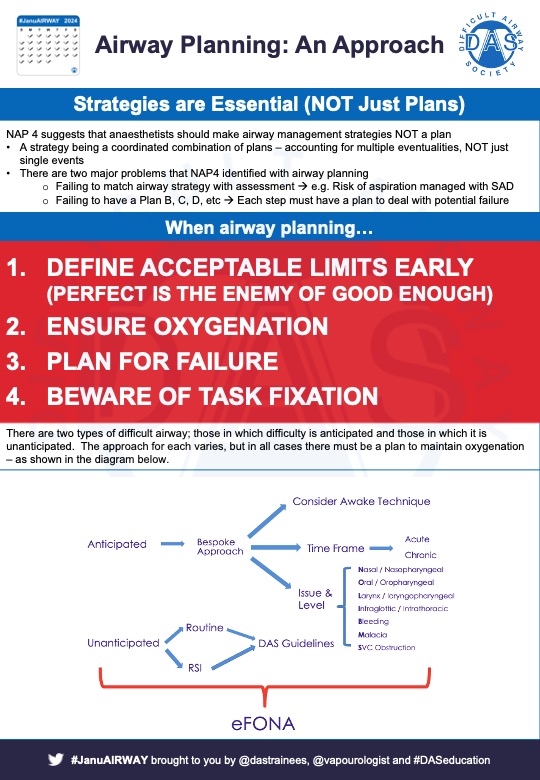
Several indications for OLV, commonest are thoracic surgery & some oesophagectomies. Essentially three ways to achieve OLV - use of:
- Double lumen tube
- Bronchial Blocker
- Elective endobronchial intubation
Here are some #OnePagers covering the basics
#JanuAIRWAY 2/9
- Double lumen tube
- Bronchial Blocker
- Elective endobronchial intubation
Here are some #OnePagers covering the basics
#JanuAIRWAY 2/9



The key physiological change is the creation of a large shunt – deoxygenated blood (which would normally be oxygenated), returns to the left heart resulting in hypoxaemia.
#JanuAIRWAY 3/9
#JanuAIRWAY 3/9

Often OLV is done in the lateral decubitus position. This has several effects on V/Q relations. As we can see in these diagrams.
#JanuAIRWAY 4/9
#JanuAIRWAY 4/9



Evolution is amazing, because we have a friend to help us deal with shunt – hypoxic pulmonary vasoconstriction. Bottom line – mechanism is complicated, it’s biphasic, aims to decrease shunt to non-ventilated lung – can be influenced by several factors.
#JanuAIRWAY 5/9
#JanuAIRWAY 5/9




Our tips for OLV:
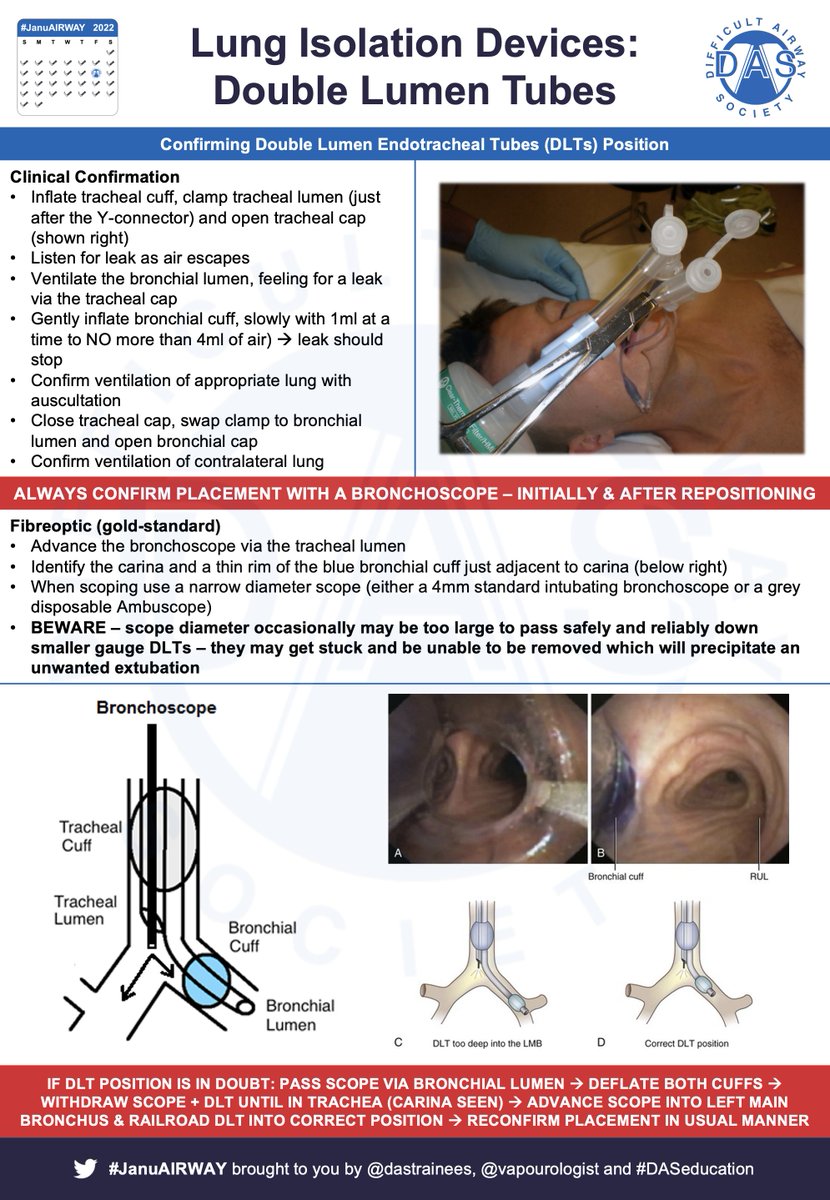
- Choose your airway wisely – get it right first time – use a fiberoptic scope
- If using bronchial blocker – consider going outside ETT.
- Be aware of physiological interplay
- Plan to deal with hypoxaemia
What’re your tips for OLV?
#JanuAIRWAY 6/9
- Choose your airway wisely – get it right first time – use a fiberoptic scope
- If using bronchial blocker – consider going outside ETT.
- Be aware of physiological interplay
- Plan to deal with hypoxaemia
What’re your tips for OLV?
#JanuAIRWAY 6/9

A knowledge of bronchoscopic anatomy is incredibly useful in anaesthesia / critical care – especially when performing OLV. Here’s a pair of #OnePagers covering the basics
#JanuAIRWAY 7/9
#JanuAIRWAY 7/9


Here are some papers / links you may find interesting:
🔗bjaed.org/article/S2058-…
🔗thoracicanesthesia.com/?page_id=2&lan…
🔗
🔗
🔗
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAIRWAY 8/9
🔗bjaed.org/article/S2058-…
🔗thoracicanesthesia.com/?page_id=2&lan…
🔗
🔗
🔗
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAIRWAY 8/9
Hope that helps. Tomorrow we'll take a look at Tracheostomies. See you then! #JanuAIRWAY 9/9
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
• • •
Missing some Tweet in this thread? You can try to
force a refresh