Here's your AB COVID # analysis for Fri Jan 14th. 1/
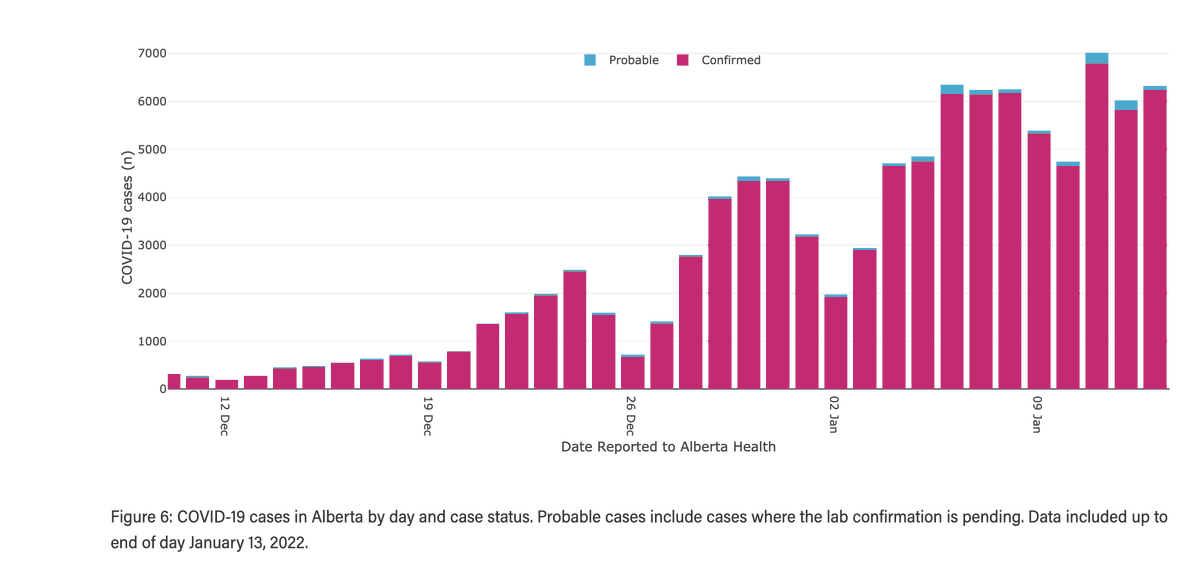
Cases/d yest 6326, a 0.2% drop from last Thurs's 6341. 7d ave now 5997 a 44.9% incr wk over wk from 4138. Positivity 37.88% compared to last Thurs 38.42% (essentially flat). Don't let the slight drop wk over wk lull you, changing test criteria make everything inaccurate. 2/ 



Hospitalizations: inpts. Last Fri +62 to 585 (revised from 681 yest 579 Wed 570 Tues 558 Mon) Sat +16 to 601 (revised from 595 yest 593 Wed 585 Tues and 555 Mon). Sun +41 to 642 (revised from 637 Yest 633 Wed 617 and Mon 563). 3/

Mon +46 to 688 (revised from 680 yest 633 Wed and 628 Tues) Tues +29 to 717 (revised from 700 yest and 666 Wed) Wed +32 to 749(revised from 707 yest). Yest -8 to 741. (subject to revision). 7d rise to Tues of 51.9% (yest 61.1% Wed 55.7% Tues 53.4% Mon 53%). 4/

I think it is really important to point out the massive revisions to the numbers of inpts. Mon for example was inititally reported at 628. today 688. These massive revisions hide rapid growth of patients. Looks like the curve is bending down, dunnit? Nope.

ICU: Wed -4 to 80 (revised from 79 yest). Yest +1 to 81. Four days of flat ICU cases is a relief. Paeds admits 6, including 2 to ICU, a 10-19year old and a baby. Total deaths 5. 6/



Demographics:Age graph:increasingly useless. See that rapid rise among the 80+? That's just b/c they meet the PCR test criteria for being vulnerable. Others don't so relatively dropping. They likely are all going straight up. Geography similarly not usefu, except relatively. 7/

Everyone I know who cares is scared and frayed. I know I am. Be kind. Forgive. We are not doing our best. Emotions are up. Love one another. We need it now more than ever. fin/
thanks to @ArynToombs @ByMatthewBlack and AB Health for the graphics.
• • •
Missing some Tweet in this thread? You can try to
force a refresh