I've seen a few people recently shouting about how new ONS data shows that the "true" death toll from COVID in England & Wales is only 17,371, rather than the ONS figure of 157,816.
This is obviously nonsense, but evidently still needs debunking, so here goes...
This is obviously nonsense, but evidently still needs debunking, so here goes...
The claim comes from an FOI request that some genius sent to the ONS asking them for the number of deaths where *only* COVID was listed on the death certificate without any other pre-existing conditions listed.
ons.gov.uk/aboutus/transp…
ons.gov.uk/aboutus/transp…
But what does it mean to die with both COVID and a pre-existing condition on the death certificate?
Death certificates list an "underlying cause" and can list several "contributory causes".
Death certificates list an "underlying cause" and can list several "contributory causes".
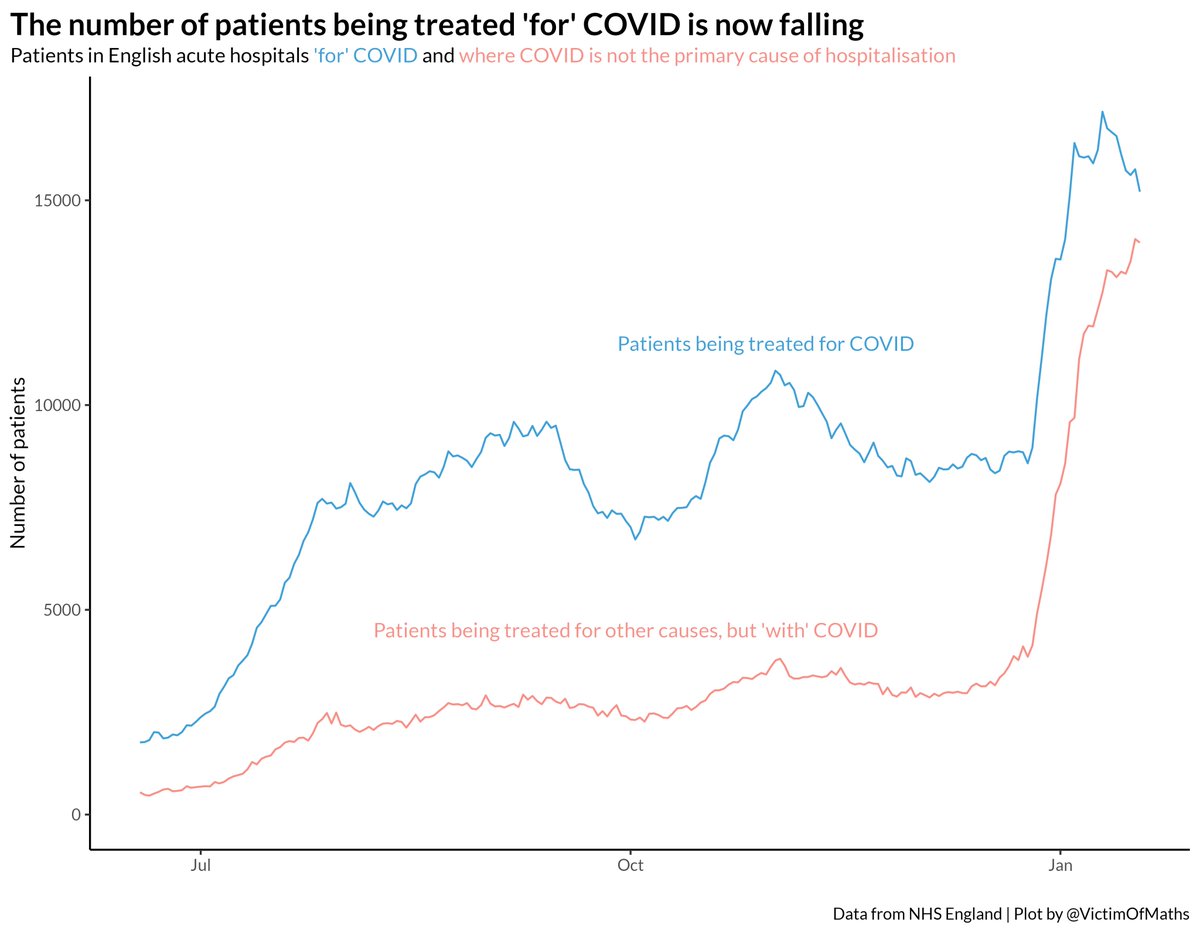
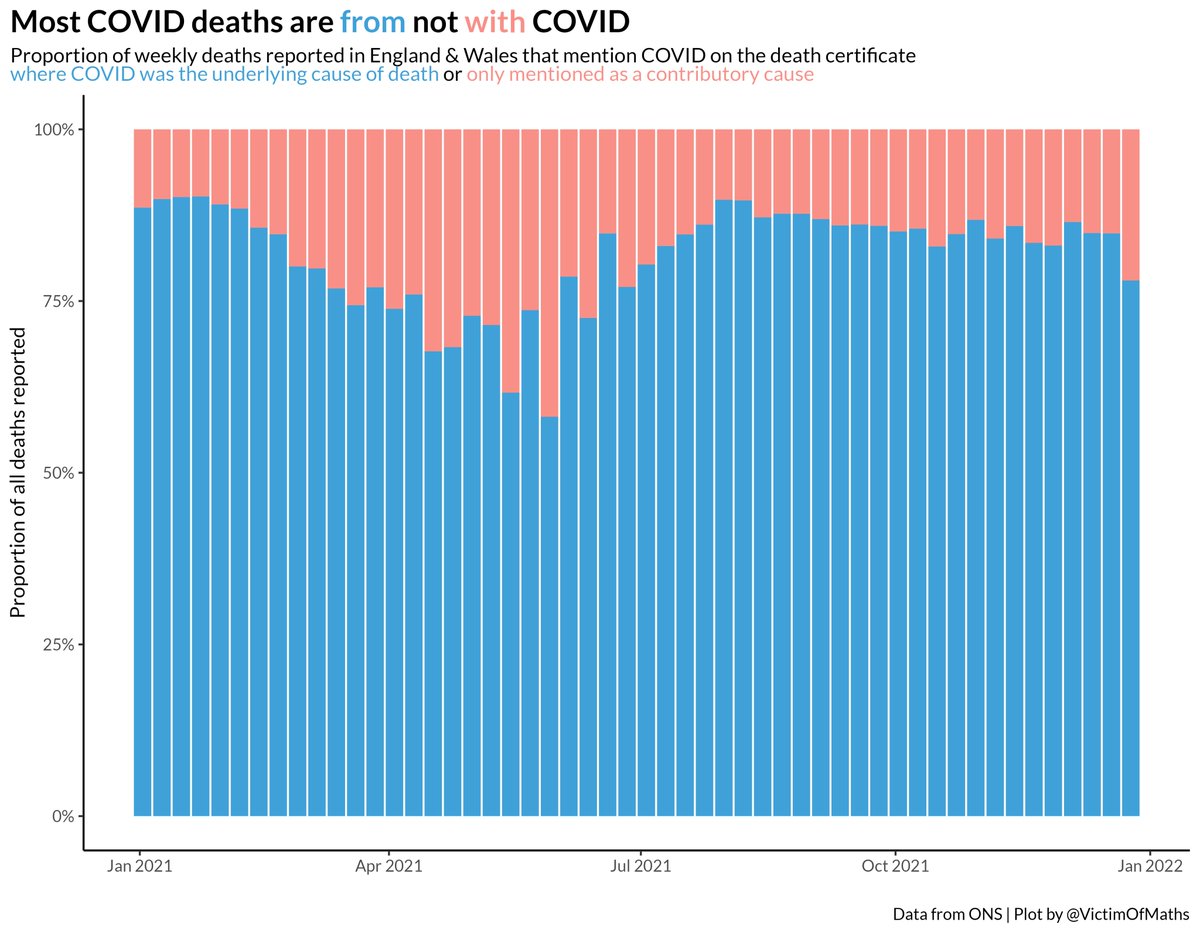
When it comes to COVID, we already know that the vast majority of deaths where COVID is mentioned on the death certificate list COVID itself as the underlying cause. 
But this new claim is that *any* deaths where there is a pre-existing condition listed on the death certificate alongside COVID aren't really COVID deaths. Because obviously these people are sick and were just about to die anyway before they caught COVID.
So what is in this list of pre-existing conditions that denote somebody who is already at death's door?
Here's the list. It is, well, pretty broad.
Here's the list. It is, well, pretty broad.
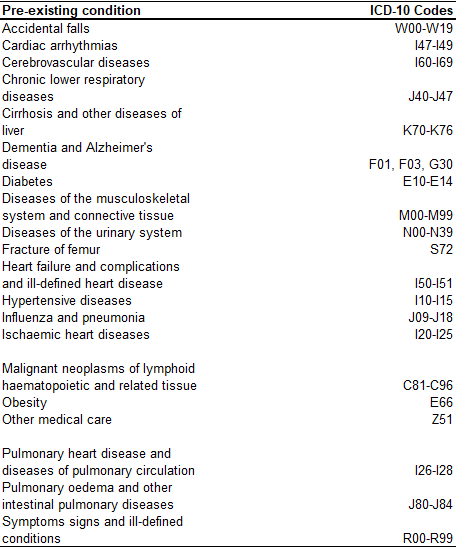
Something like a third of the population have high blood pressure (hypertension), ~5 million people in the UK have diabetes, just under a third are obese etc. etc.
And prevalence of these conditions is strongly linked to age. Slightly different definition (though similar), but here's a great study from Scotland on the prevalence of long-term health conditions by age.
thelancet.com/journals/lance…
thelancet.com/journals/lance…
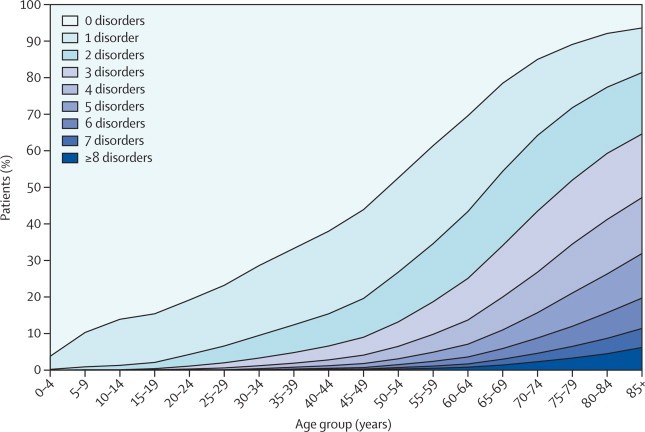
Once you get past your mid-50s, chances are you have a long-term health condition. By the time you reach your 70s, you have to be extremely lucky not to.
So that is a *lot* of people with pre-existing conditions. If any of them were unlucky enough to have caught COVID, get severely ill and die, all it takes is for these conditions to have *some* impact for it to end up as a contributory cause on the death certificate.
To illustrate how stupid this whole argument is, let's take an example - asthma. The ICD-10 code for asthma is J45, so it's on the list of pre-existing conditions.
COVID is a respiratory virus. Many of the people who get severely ill have trouble breathing and need ventilation. It is hopefully obvious that having asthma will potentially exacerbate these difficulties and will therefore be listed as a contributory cause if they sadly die.
It seems extremely bizarre to claim that this means the person died from asthma and not from COVID. Perhaps they wouldn't have died if they didn't have asthma, but they *definitely* wouldn't have died if they didn't have COVID.
Not counting deaths with pre-existing conditions is saying to people with these conditions that their lives don't matter.
The argument being made is that only the lives of people with no pre-existing health conditions count.
The argument being made is that only the lives of people with no pre-existing health conditions count.
This is obviously repugnant. It's the even nastier cousin of the 'they were old and would have died soon anyway' argument that we've heard trotted out many times, in spite of the fact that the average years of lost life per COVID death is ~10.
wellcomeopenresearch.org/articles/5-75
wellcomeopenresearch.org/articles/5-75
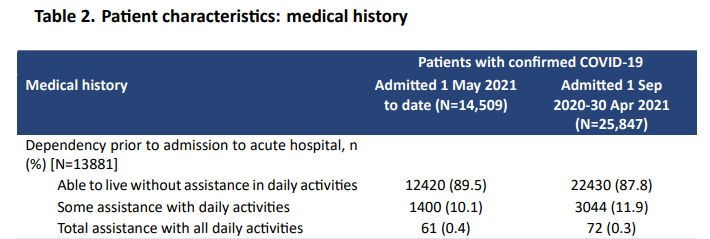
Data from ICNARC shows that the vast majority of people being admitted to critical care were happily living without any support prior to admission.
These are not people who were already at death's door.
icnarc.org/our-audit/audi…
These are not people who were already at death's door.
icnarc.org/our-audit/audi…
People with pre-existing conditions are real people. Their lives matter. They are your parents, your grandparents, your friends, your children. Very possibly you.
If you are seriously making the argument that only 17,371 people have *really* died from COVID then you are saying that the ~140,000 people who died with pre-existing conditions were expendible and didn't matter.
I hope it's obvious that that is an utterly repulsive and morally indefensible position.
Don't even *think* about trying to make that argument to me.
Don't even *think* about trying to make that argument to me.
As a final comment, there was absolutely no need for anyone to have FOIed this data. It was already in the public domain, published quarterly here:
ons.gov.uk/peoplepopulati…
ons.gov.uk/peoplepopulati…
But I think it says a lot about the kind of person making these arguments that rather than go and look for the data to answer a question, their first resort of just to send an FOI request demanding somebody provide it to them on a plate.
• • •
Missing some Tweet in this thread? You can try to
force a refresh