
Kids desperately need normal life back. To support everyone trying to understand the overall best for them right now, we've created this Advocacy Toolkit. It boils down the data on vaccines, Omicron, and mental health to advocate for kids as whole people. urgencyofnormal.com 

The toolkit is an independent collaboration of diverse voices from the medical community. Its origins came from partnering with our own children's schools to help them make sense of the data and make wise choices.

Although there are many articles written about COVID, there wasn't one simple place that integrates and balances all the critical data needed for parents, students, teachers, and mentors to make the decisions they're facing right now. This toolkit was created to meet that need.

Who is this for? Everyone with a role to play in caring for our kids and schools. Please use it with compassion and understanding. We've all been through a lot.

We CAN give our children normal life back while also protecting the vulnerable, and letting go of policies that are not supported by data. In fact, we must- because the impacts on our children's overall health from two years of disruption are too grave to continue.

First, calibrate the actual risk level for kids. It's not zero, but it isn't extraordinary either. We never disrupted our children's lives like this for the flu, because we knew the unintended consequences would be too many and too damaging.

With vaccination, that low risk is driven much further down, to far below flu-like levels.

Thankfully, Omicron does not change the severe disease risk for kids. It spreads faster, but vaccines continue to prevent severe disease with amazing effectiveness.

We understand that many adults are nervous about their own health too. Boosters are remarkably effective for keeping high-risk groups protected, again reducing risk to flu-like levels or below.

Meanwhile, our children's mental health is in crisis. The data are staggering, with many millions of children affected. The consequences can be severe, even fatal. The path we are on is too dangerous to continue.

School closures need to end and never be repeated. "The toll of school closures and social isolation on children's mental health cannot be overstated." -JAMA Pediatrics Editorial

Giving normalcy back to children doesn't mean abandoning those vulnerable to COVID. Focused protection measures can keep them safe. We've used them our whole lives to protect immunocompromised people from the flu, and they're MORE effective than "my mask protects you."

The data lead us to this: re-establishing fully normal life for children is urgent. De-escalate fear and tell children how safe they are. Use boosters to protect the elderly and high-risk, and focused protection measures for those for whom vaccination is not enough.

We're calling for a change in mindset. If we stop viewing COVID as the only thing that kids need protection from, we'll see them as whole people and make balanced choices to support them and help them thrive.

Appendix: Student masking is the most visible and controversial ongoing school COVID mitigation, so it's important to empower people with the real-world data on mask effectiveness.

What matters is effectiveness in the real world. There are 5 well-controlled real world studies that evaluate student masking. All find the same result: any benefit, if it exists, is too small to confidently detect. This includes studies from the CDC and the UK government.
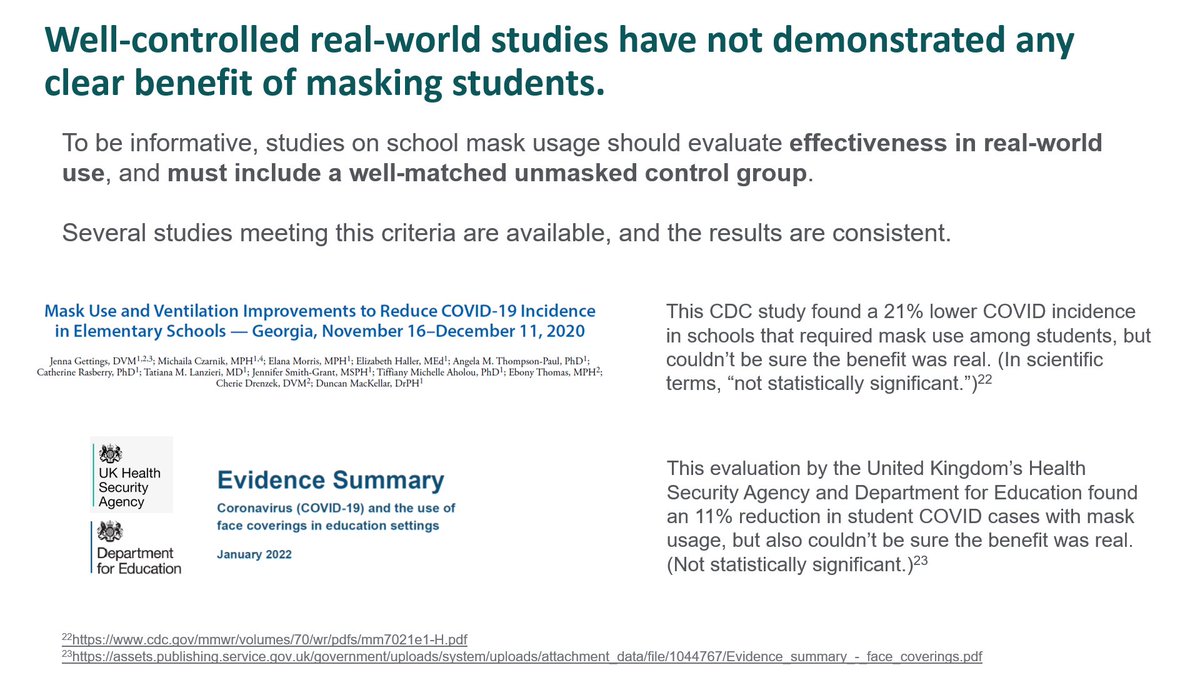
Academic studies find the same result.

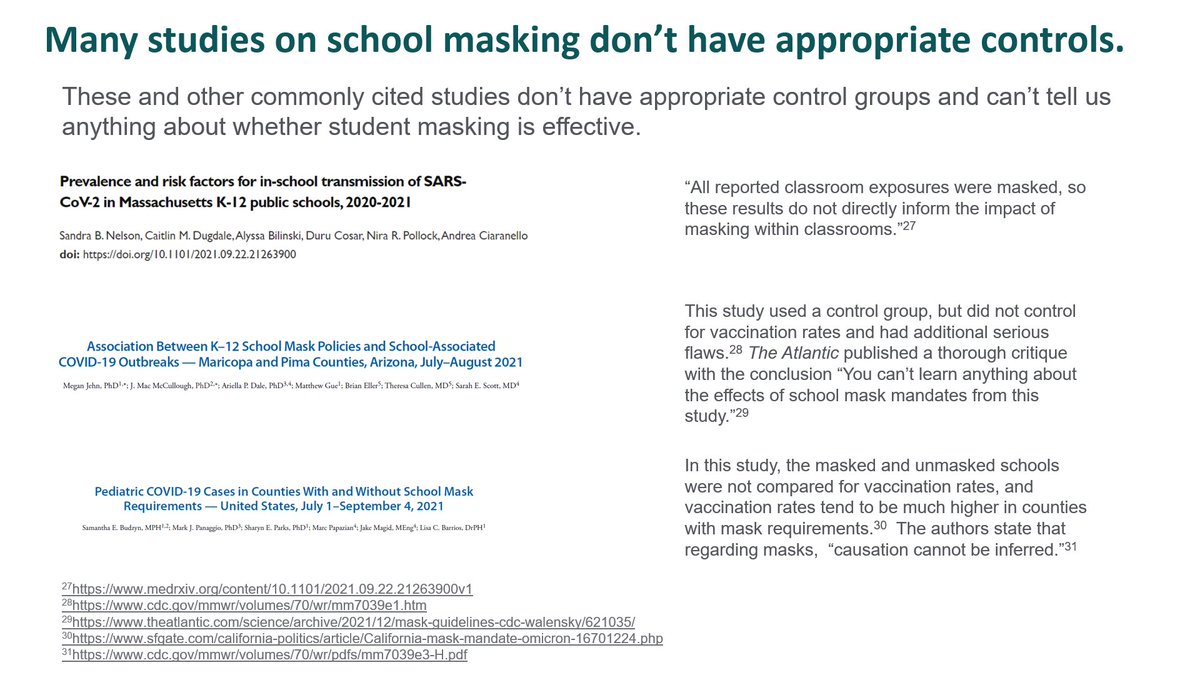
In contrast to the well-designed studies above, studies often cited to support student masking lack appropriate control groups. Some of the most prominent are cited here, with quotes and links to critiques from other scientists.
This is why Focused Protection is so important: it actually works. It is dangerous to send vulnerable children, or children with vulnerable family members, out with the belief that other people's masks protect them, when the data shows little or no effectiveness.

Student masking: when an intervention's real-world benefits are too small to measure, we should feel comfortable ending its use. Acknowledging that dropping masks is a big shift for many, we call for a change to mask-optional everywhere no later than Feb 15th.

Our goal is to empower you with the data, so we've included links to all of the data sources throughout the toolkit. Suspicious of our interpretation? Go double-check us, we've made it easy.
As scientists and physicians, our goal is to provide accurate data and nuanced guidance—to help people frame decisions and balance risk—not to make decisions for you. We hope this toolkit is a benefit to you, your community, and your children. urgencyofnormal.com
My co-authors on Twitter: @MonicaGandhi9 @drlucymcbride @TracyBethHoeg @JeanneNoble18 @kwadwo777 @JVergales @notaproviderMD @doctortara @DrAmyBeck
Download the toolkit in PDF form at urgencyofnormal.com
Update 1/26: Thanks to constructive feedback, we made refinements to our toolkit that differ from some of the images shown above. Please download the latest version to get the most accurate information. urgencyofnormal.com
• • •
Missing some Tweet in this thread? You can try to
force a refresh














