Brief update on Omicron, and its BA.1 and BA.2 lineages (sisters)
1. Origin—the 3 theories for how this hyper-mutated version of the virus evolved
nature.com/articles/d4158… @nature
1. Origin—the 3 theories for how this hyper-mutated version of the virus evolved
nature.com/articles/d4158… @nature

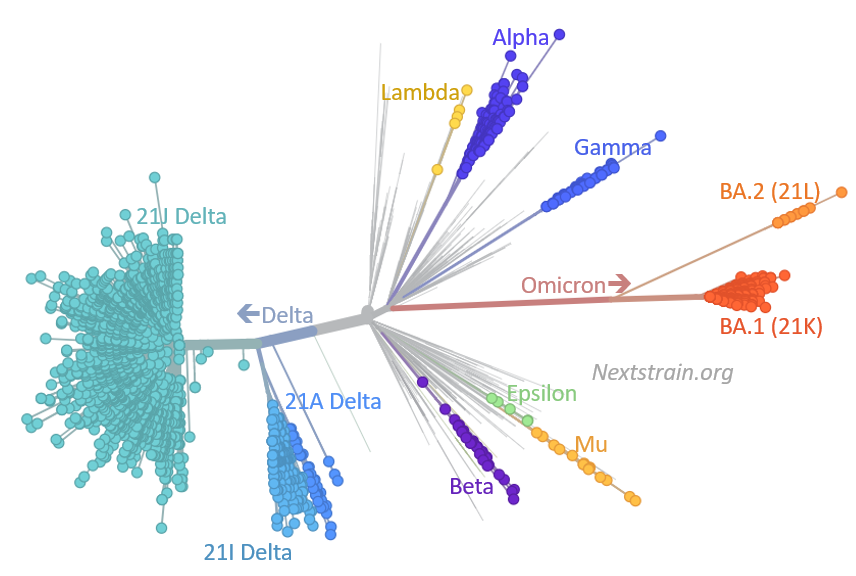
2. A great annotated graphic by @firefoxx66 of @nextstrain conveying the antigenic distance of Omicron's BA.1 and BA.2 from prior variants
nextstrain.org/ncov/gisaid/gl…
nextstrain.org/ncov/gisaid/gl…
3. The BA.2 variant is spreading widely, throughout many countries in Europe and Asia, out-competing BA.1, indicating higher transmissibility. But the good news from yesterday's @UKHSA: vaccination + boost is holding up quite well; there's no indication of more immune evasion

4. Some countries where BA.2 (light purple) is making or has already made major inroads outcompeting BA.1 (purple) covariants.org

5. And there's a new thread from @trvrb covering these points and many others, with the conclusion that BA.2's impact of extending the length of time (longer tail) for the Omicron wave
https://twitter.com/trvrb/status/1487105396879679488
7. A new BA.2 dedicated report today from @UKHSA
The secondary attack rate for BA.2 compared with BA.1 is roughly 30% increased, reflecting a transmission edge
assets.publishing.service.gov.uk/government/upl…
And another invaluable @kallmemeg🧵takes you through the rest of it
The secondary attack rate for BA.2 compared with BA.1 is roughly 30% increased, reflecting a transmission edge
assets.publishing.service.gov.uk/government/upl…
And another invaluable @kallmemeg🧵takes you through the rest of it
https://twitter.com/kallmemeg/status/1487157510448549891

• • •
Missing some Tweet in this thread? You can try to
force a refresh