Here's your AB COVID # analysis for Tues Feb 8th. 1)
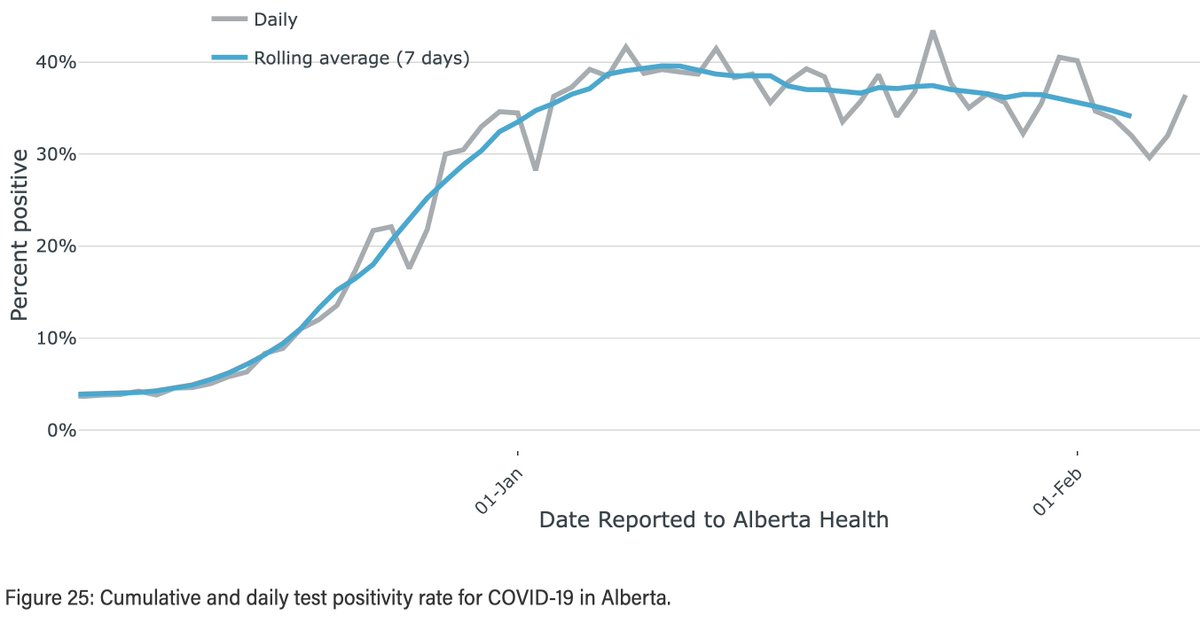
CAses/d (I know y'all know this fact, but for those who don't (@jkenney) this is a pretty useless metric now that testing is restricted) 1773. Positivity 36.43% (last Mon 40.53%). 2/ 

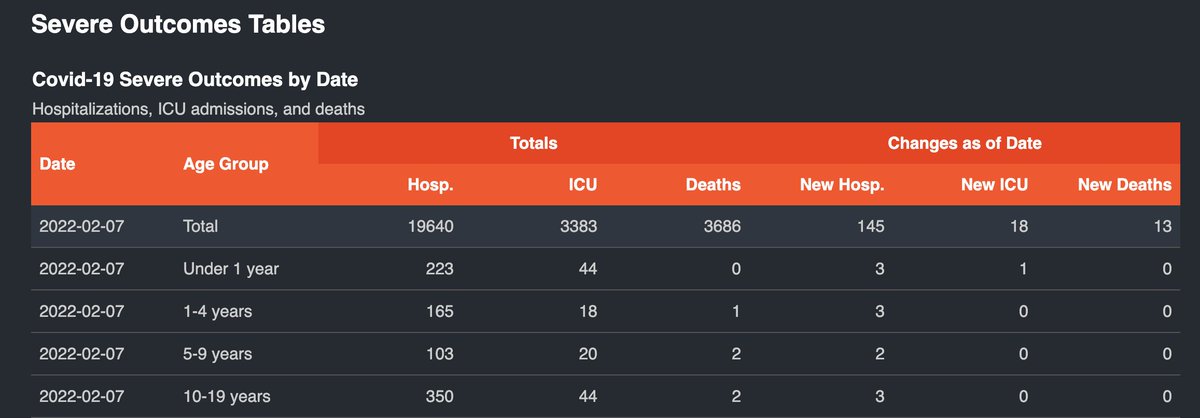
Hospitalization: Inpt: Last Tues +22 to 1568 (new pandemic record) (revised from 1566 yest 1554 Fri 1542 Thurs and 1492 Wed) Wed -35 to 1533 (revised from 1530 yest 1515 Fri and 1472 Thurs) Thurs -21 to 1512(revised from 1507 yest and 1466 Fri). 3/

Fri -14 to 1498 (revised from 1492 yest), Sat -48 to 1450 (revised from 1437 yest), Sun +26 to 1476 (Revised from 1424 yest). yest +18 to 1494 (subj to revision) ICU: Sun +2 to 119 (revised from 118 yest) Yest +10 to 128 (new #weararespiratorwave record) (subj to revision). 5/

Paeds admits 11, incl one baby in the ICU. Deaths 13 (we've been bouncing around 13-15 deaths/day for quite a while). 6/

Finishing up with some rural wastewater monitoring graphs. It may be dropping in urban areas, but rural areas are another thing altogether. Source: covid-tracker.chi-csm.ca fin/




thanks to @ArynToombs and AB Health for the graphics.
• • •
Missing some Tweet in this thread? You can try to
force a refresh