
1/
Let's be honest...
💥💥“THE TISSUE IS THE ISSUE” 💥💥
#Nephropath #NephMadness
This region features:
🔎PLA2R 🆚Other Membranous Antigens
🔎DNAJB9 🆚IgG4 Disease
READY???👇👇
ajkdblog.org/2022/03/01/nep…
Let's be honest...
💥💥“THE TISSUE IS THE ISSUE” 💥💥
#Nephropath #NephMadness
This region features:
🔎PLA2R 🆚Other Membranous Antigens
🔎DNAJB9 🆚IgG4 Disease
READY???👇👇
ajkdblog.org/2022/03/01/nep…
2/
Matchup 1⃣: PLA2R 🆚Other MN Antigens
PLA2R facts
✅Present in healthy human podocytes
✅70-80% 👥with 1ry MN & ~ 60% of ALL MN
✅Serum Ab are measured via ELISA & IF
💡💡DX:
🧪ELISA > 14 RU/mL or
🧪ELISA 2 - 14 RU/mL WITH a positive IFA
pubmed.ncbi.nlm.nih.gov/34556256/
Matchup 1⃣: PLA2R 🆚Other MN Antigens
PLA2R facts
✅Present in healthy human podocytes
✅70-80% 👥with 1ry MN & ~ 60% of ALL MN
✅Serum Ab are measured via ELISA & IF
💡💡DX:
🧪ELISA > 14 RU/mL or
🧪ELISA 2 - 14 RU/mL WITH a positive IFA
pubmed.ncbi.nlm.nih.gov/34556256/
3/
Check this beautiful Visual Abstract by @Vernisartan on the serology based approach to MN
A few more words on Anti-PLA2R titers:
✅>150 RU/mL- ⏫ risk of progression
✅> 45 RU/mL- ⏫risk of recurrence post transplant
💡 Titers are part of the risk stratification algorithm💡
Check this beautiful Visual Abstract by @Vernisartan on the serology based approach to MN
A few more words on Anti-PLA2R titers:
✅>150 RU/mL- ⏫ risk of progression
✅> 45 RU/mL- ⏫risk of recurrence post transplant
💡 Titers are part of the risk stratification algorithm💡

4/
Why do the other MN antigens matter❓
MN antigens:
✅Have different disease associations
✅Are challenging the old nomenclature of 1ry & 2ry MN
✅Opened the door for research on antigen specific therapies
Why do the other MN antigens matter❓
MN antigens:
✅Have different disease associations
✅Are challenging the old nomenclature of 1ry & 2ry MN
✅Opened the door for research on antigen specific therapies

5/
Matchup 2⃣: DNAJB9🆚IgG4
DNAJB9 facts:
✅~💯 sensitivity & specificity for FIBRILLARY GN
✅🔬EM: ~20 nm randomly organized fibrils
✅44% of 👥progress to ESKD within 4 years
✅Tx: ❓ 1/3 of patients respond to rituximab
Check this wonderful VA by @iheartkidneys
Matchup 2⃣: DNAJB9🆚IgG4
DNAJB9 facts:
✅~💯 sensitivity & specificity for FIBRILLARY GN
✅🔬EM: ~20 nm randomly organized fibrils
✅44% of 👥progress to ESKD within 4 years
✅Tx: ❓ 1/3 of patients respond to rituximab
Check this wonderful VA by @iheartkidneys

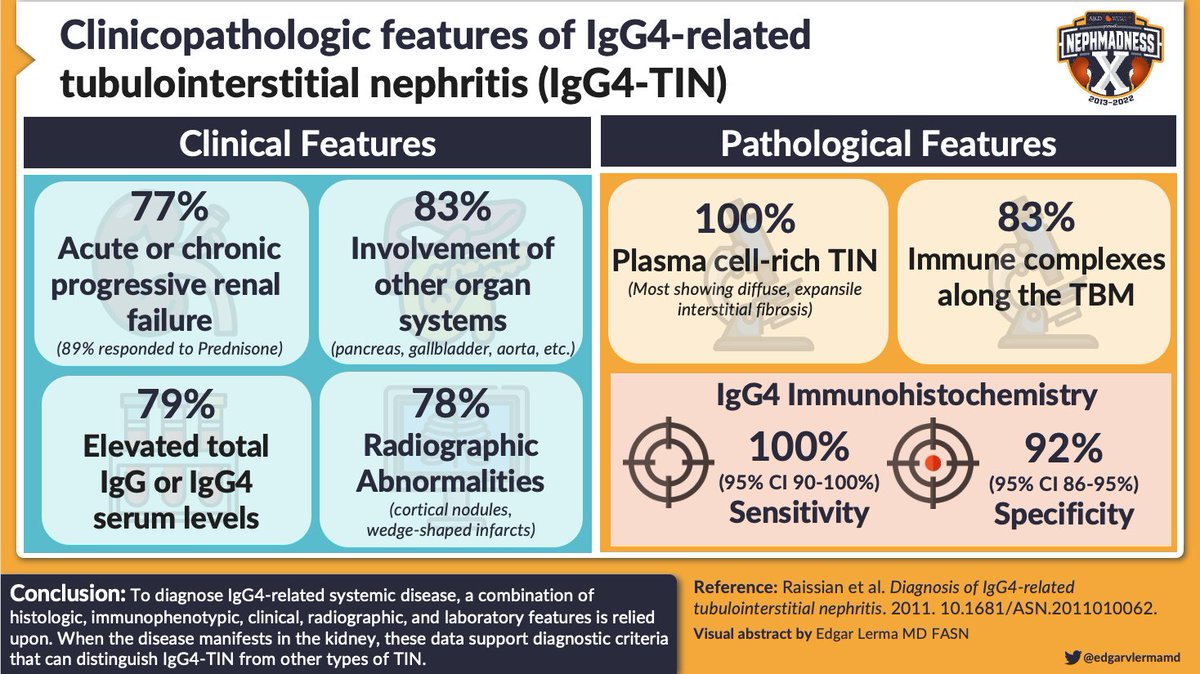
6/
IgG4 facts:
✅Tubulointerstitial nephritis is the most common kidney manifestation
✅🔬PAS & Silver stain: "storiform fibrosis" is characteristic
✅Excellent response to steroids -- & 20% relapse
Check this amazing VA by @edgarvlermamd
IgG4 facts:
✅Tubulointerstitial nephritis is the most common kidney manifestation
✅🔬PAS & Silver stain: "storiform fibrosis" is characteristic
✅Excellent response to steroids -- & 20% relapse
Check this amazing VA by @edgarvlermamd
Thank you @nephrosharma @Maximal_Change @Khairallah_P @Nephro_Sparks @arkanalabs for inviting me to be part of this fun region and for your feedback! #NephMadness

• • •
Missing some Tweet in this thread? You can try to
force a refresh



