
When was the last time you saw a pt with hepatic encephalopathy or lost a pt to cerebral edema from it?
Ever wondered why liver failure causes HE & Cerebral edema? What if conventional Rx fail?
If interested in journey to MARS, keep reading.
Bringing awareness to #neurologists.
Ever wondered why liver failure causes HE & Cerebral edema? What if conventional Rx fail?
If interested in journey to MARS, keep reading.
Bringing awareness to #neurologists.

Pt w/ MVA,G5 liver lac,hepatic art sacrificed,LFT 5k,NH3 250,GCS 4
Pt w/🍺cirrhosis,found down,severe rhabdo,CK📈,NH3 400s,renal shutdown,GCS 5
Pt w/ colon Ca on @KEYTRUDA w/jaundice DILI
Pt w/ liver transplant, p/w intractable pruritus
You got the gist-MARS aka Albumin dialysis
Pt w/🍺cirrhosis,found down,severe rhabdo,CK📈,NH3 400s,renal shutdown,GCS 5
Pt w/ colon Ca on @KEYTRUDA w/jaundice DILI
Pt w/ liver transplant, p/w intractable pruritus
You got the gist-MARS aka Albumin dialysis
Pathyphysiology of cerebral edema in HE.
An article by @EWijdicks elegantly describes it. (PMID:27783916)
In Liver failure (LF), ⬆️NH3 cross BBB, converted to glutamine👉🏻osmotic gradient and CE.
Risk of cerebral edema (CE) ⬆️ with NH3 >200 micro moles/L.
An article by @EWijdicks elegantly describes it. (PMID:27783916)
In Liver failure (LF), ⬆️NH3 cross BBB, converted to glutamine👉🏻osmotic gradient and CE.
Risk of cerebral edema (CE) ⬆️ with NH3 >200 micro moles/L.

Here is the toxin hypothesis of vicious cycle that occurs in LF, can lead to CE + herniation.
Basically states that liver injury does not only impair toxin clearance but also can cause impaired hepatic regeneration 👉🏻 further exacerbation of LF + toxin clearance. (PMID:22228886)
Basically states that liver injury does not only impair toxin clearance but also can cause impaired hepatic regeneration 👉🏻 further exacerbation of LF + toxin clearance. (PMID:22228886)

Rx for ICP:hypertonic,sedation,🤷🏻♂️from now on #verticalization @namorrismd
Last resort👉🏻may need Extracorporeal Liver Support-ECLS👉🏻3 goals:
✅remove toxin
✅synthesize protein
✅reverse inflamm by cytokines
MARS=Molecular Adsorbant Recirculating System👉🏻1 of many ways of ECLS.
Last resort👉🏻may need Extracorporeal Liver Support-ECLS👉🏻3 goals:
✅remove toxin
✅synthesize protein
✅reverse inflamm by cytokines
MARS=Molecular Adsorbant Recirculating System👉🏻1 of many ways of ECLS.

ECLS are of 2 main types; (25438293,26311600)
Type 1:Artificial/acellular/non-biologic:Utilize artificial membrane 👉🏻adsorption+detoxification of🩸
Pros:
✅easy 2 use
✅reverses pathyphysiology of LF
✅cheap
Cons:
☑️no synthetic func
E.g.MARS (main focus here), SPAD, Prometheus
Type 1:Artificial/acellular/non-biologic:Utilize artificial membrane 👉🏻adsorption+detoxification of🩸
Pros:
✅easy 2 use
✅reverses pathyphysiology of LF
✅cheap
Cons:
☑️no synthetic func
E.g.MARS (main focus here), SPAD, Prometheus

Type 2:Bio-artificial/Cellular/Biologic:Utilize live hepatocytes from human or 🐷 source soaked in a medium in cartridge through which🩸is passed for detoxification.
Pros:
✅+synthetic func
Cons:
☑️complex technology
☑️cell source supply issue
☑️Xenotransmission
☑️💰💵🤑
Pros:
✅+synthetic func
Cons:
☑️complex technology
☑️cell source supply issue
☑️Xenotransmission
☑️💰💵🤑

We use MARS @EmoryGastroHep @EmoryCCC @EmoryPCCM @EmoryNeuroCrit
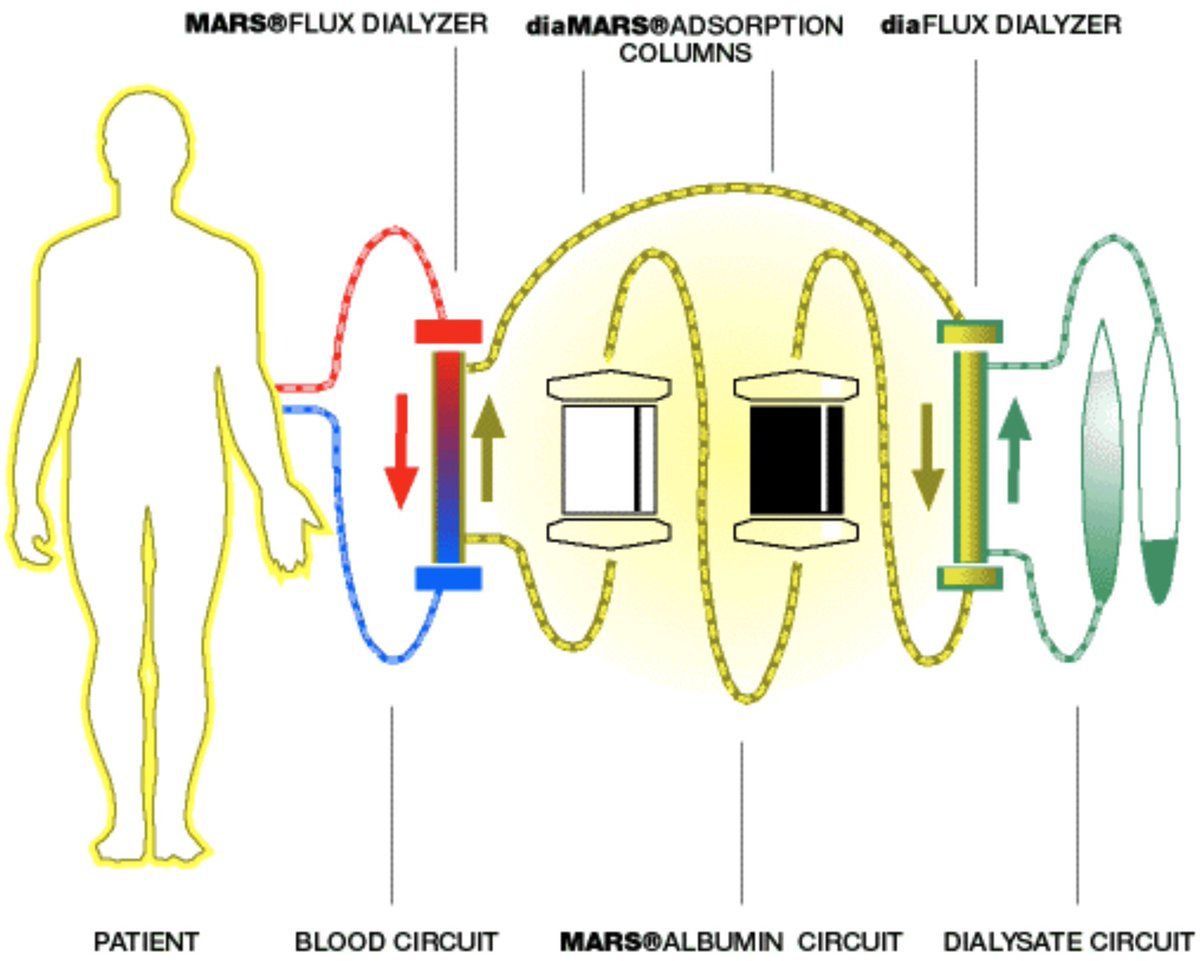
MARS has 2 different circuits merged together:
🟡albumin dialysate high-flux dialyzer(protein-bound ☠️+cytokine+drugs)
🟢renal dialysate low-flux filter(water sol☠️)
Basically,add albumin circuit b/w blood & CRRT
MARS has 2 different circuits merged together:
🟡albumin dialysate high-flux dialyzer(protein-bound ☠️+cytokine+drugs)
🟢renal dialysate low-flux filter(water sol☠️)
Basically,add albumin circuit b/w blood & CRRT
🛑for a sec.
Understand Dalton-unit of atomic mass of an atom in reference to C-12(g/mol)
For filter, 1000Da (1 kDa) =1.3nm pore size. 35 kDa filter allows everything <=35 kDa size to pass through.
Ammonia=17Da
Urea=60Da
Cr=113Da
Bile acid=500Da
Albumin=67 kDa
DNA=~156 billionDa
Understand Dalton-unit of atomic mass of an atom in reference to C-12(g/mol)
For filter, 1000Da (1 kDa) =1.3nm pore size. 35 kDa filter allows everything <=35 kDa size to pass through.
Ammonia=17Da
Urea=60Da
Cr=113Da
Bile acid=500Da
Albumin=67 kDa
DNA=~156 billionDa
Molecules cleared by MARS:
Water soluble-NH3, Urea, Creatinine, (?? nitric oxide👉🏻improved hemodynamics)
Protein-bound-Bilirubin (indirect), Bile acid, Tryptophan, Fatty acids(low, medium chain), TNF & IL(CK), Cu, BZD & drugs.
Here’s, what happens across the filter membrane.
Water soluble-NH3, Urea, Creatinine, (?? nitric oxide👉🏻improved hemodynamics)
Protein-bound-Bilirubin (indirect), Bile acid, Tryptophan, Fatty acids(low, medium chain), TNF & IL(CK), Cu, BZD & drugs.
Here’s, what happens across the filter membrane.

What do you need to start MARS circuit?
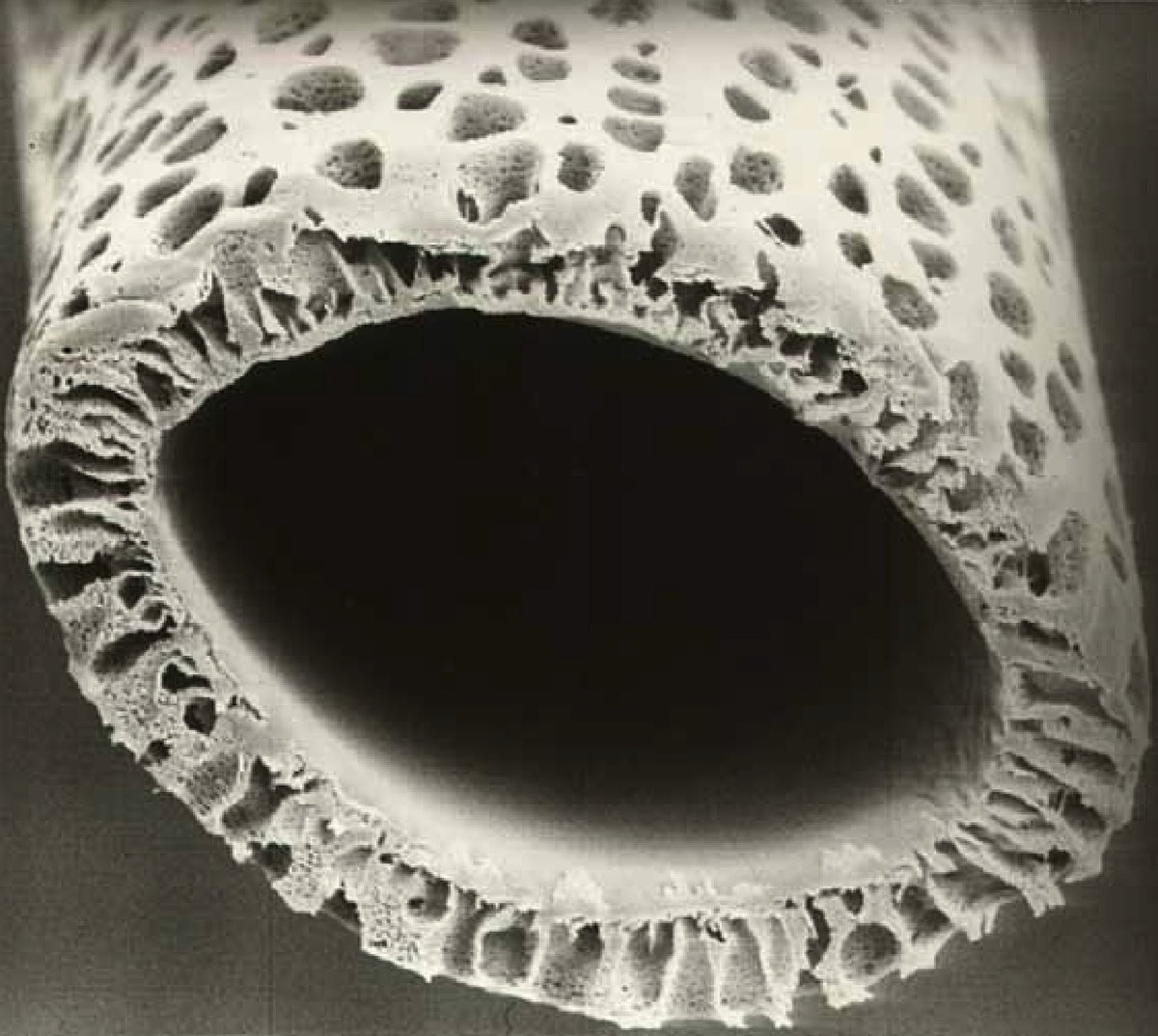
1. High-flux dialyzer(HFD)
Surface area=2.1m2
Mol size cut off=50kDa(🧘we won’t loose pt’s Albumin)
✅removes Alb-bound☠️ from 🩸
Hollow fiber compart-pt’s🩸,dialysate compart-Albumin dialysate(600cc 16% Albumin=400cc 25% Alb+200cc NS)
1. High-flux dialyzer(HFD)
Surface area=2.1m2
Mol size cut off=50kDa(🧘we won’t loose pt’s Albumin)
✅removes Alb-bound☠️ from 🩸
Hollow fiber compart-pt’s🩸,dialysate compart-Albumin dialysate(600cc 16% Albumin=400cc 25% Alb+200cc NS)

2. Low-flux dialyzer(LFD)
Surface area=1.4m2
Mol size cut off=30-35kDa
✅removes water sol☠️-NH3,Urea,Cr from used Albumin dialysate
Hollow fiber compartment- Used toxin rich albumin dialysate, Dialysate compartment-bicarb based renal dialysate.
Surface area=1.4m2
Mol size cut off=30-35kDa
✅removes water sol☠️-NH3,Urea,Cr from used Albumin dialysate
Hollow fiber compartment- Used toxin rich albumin dialysate, Dialysate compartment-bicarb based renal dialysate.

3.MARS Ion exchanger resin cartridge(IE250)
Adsorbant cartridge w/ ion exchanger resin
✅removes anionic molecules e.g.bilirubin
4.MARS Activated charcoal cartridge(AC250)
Adsorbant cartridge w/ activated charcoal
✅removes low-molecular, non-polar☠️e.g.fatty acid,bile acid
Adsorbant cartridge w/ ion exchanger resin
✅removes anionic molecules e.g.bilirubin
4.MARS Activated charcoal cartridge(AC250)
Adsorbant cartridge w/ activated charcoal
✅removes low-molecular, non-polar☠️e.g.fatty acid,bile acid


5.Particle filter(PF)
6.Two different dialysate (albumin and bicarbonate based renal)
7.CRRT machine
✅pumps pt’s 🩸and renal dialysate circuit
8. MARS machine
✅pumps albumin dialysate circuit through HFD
9. Central venous access with VasCath / Trialysis
6.Two different dialysate (albumin and bicarbonate based renal)
7.CRRT machine
✅pumps pt’s 🩸and renal dialysate circuit
8. MARS machine
✅pumps albumin dialysate circuit through HFD
9. Central venous access with VasCath / Trialysis



Now since we have all pieces together, let’s make a MARS circuit:
Hint:
Green-simplified renal dialysate circuit
Black/yellow-albumin dialysate circuit (black=used albumin, shades of yellow=dark to bright,more cleaner albumin.
Red-pt’s 🩸with toxins
Blue-pt’s 🩸free of toxins
Hint:
Green-simplified renal dialysate circuit
Black/yellow-albumin dialysate circuit (black=used albumin, shades of yellow=dark to bright,more cleaner albumin.
Red-pt’s 🩸with toxins
Blue-pt’s 🩸free of toxins
✅🩸only passes through HFD,not LFD.
✅Used Albumin dialysate from HFD is diverted to LFD first to filter water sol☠️ before going to MARS PF, AC & IE filters for recycling.
✅pt’s Albumin never gets filtered, nor does it make contact w/ dialysate Albumin.
✅Used Albumin dialysate from HFD is diverted to LFD first to filter water sol☠️ before going to MARS PF, AC & IE filters for recycling.
✅pt’s Albumin never gets filtered, nor does it make contact w/ dialysate Albumin.

✅since we’re running 2 circuits(Alb dialysate+renal dialysate) w/ 2 machines (MARS+CRRT) in a single continuum, the flow rates must be the same in both machines. 150-200ml/min(usually 180)
✅circuit needs to be primed ~2 hrs before anticipated use.
✅don’t forget heparin/citrate
✅circuit needs to be primed ~2 hrs before anticipated use.
✅don’t forget heparin/citrate
Duration of Rx=6-8hrs, max 10. Why?
👉🏻potential risk of Alb becoming culture medium w/ longer use
👉🏻AC & IE filters get saturated after 6-8hrs
✳️Usually 3-5 sessions are done, may be more.
✳️MARS is not a destination treatment, it’s bridge to spontaneous recovery or transplant
👉🏻potential risk of Alb becoming culture medium w/ longer use
👉🏻AC & IE filters get saturated after 6-8hrs
✳️Usually 3-5 sessions are done, may be more.
✳️MARS is not a destination treatment, it’s bridge to spontaneous recovery or transplant
So what’s in it for 🧠👨⚕️?
We must know when to anticipate MARS in pt w/ HE and understand it’s effects on 🧠& recovery.
1.Effects on hemodynamics:
Confounded data but some suggest improved MAPs,others not. Almost everyone found improved SVR (may be nitric oxide clearance?)
We must know when to anticipate MARS in pt w/ HE and understand it’s effects on 🧠& recovery.
1.Effects on hemodynamics:
Confounded data but some suggest improved MAPs,others not. Almost everyone found improved SVR (may be nitric oxide clearance?)

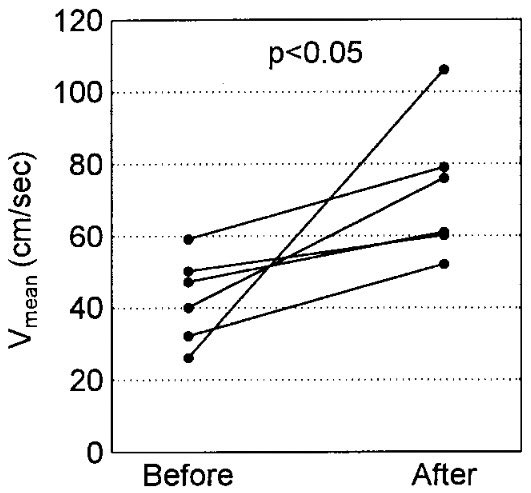
2.Effects on CBF, 🧠O2 consumption:
✳️⬆️ Vmean in MCA w/ TCD (12950955)
✳️⬇️SjVO2(jug venous O2) from 86%->70%,marker of 🧠O2 consumption.
✳️Average ⬆️GCS by 4-6,independent of survival (11445681)
One study reported 5/8 pts improved from comatose to GCS>13 after just 1 Rx MARS
✳️⬆️ Vmean in MCA w/ TCD (12950955)
✳️⬇️SjVO2(jug venous O2) from 86%->70%,marker of 🧠O2 consumption.
✳️Average ⬆️GCS by 4-6,independent of survival (11445681)
One study reported 5/8 pts improved from comatose to GCS>13 after just 1 Rx MARS


3.Effects on ICP & HE:
✳️⬇️⬇️ICP from 37 to 13 on average (12602522) & resolution of CE on CT.
✳️average ⬇️ HE grade by 2 (West Haven)
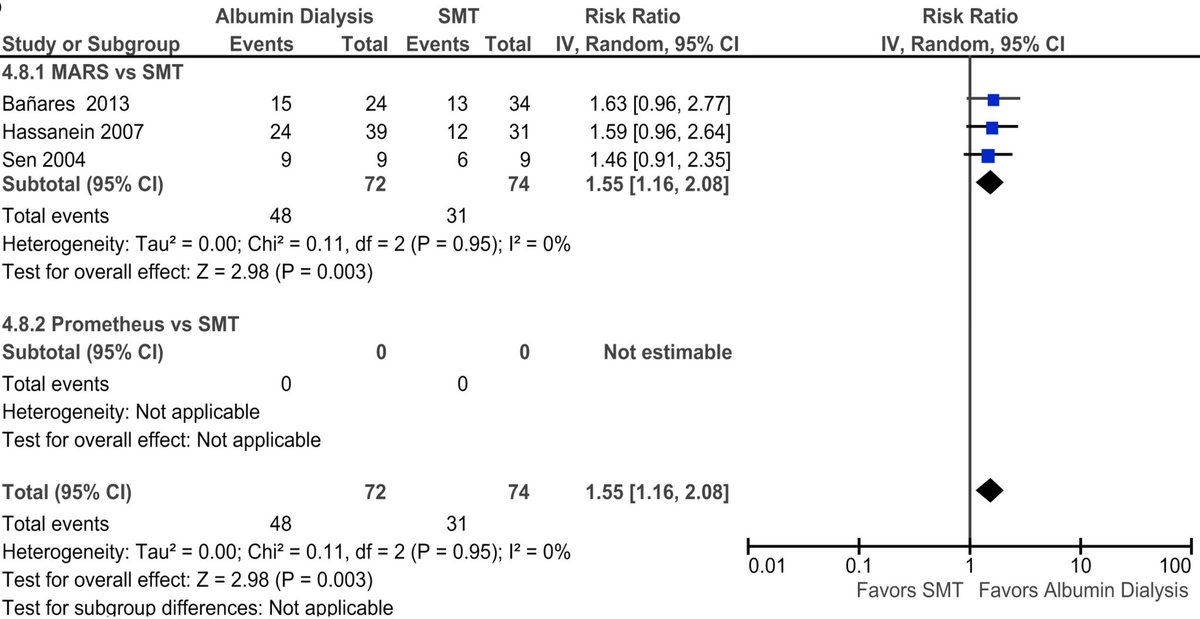
✳️55% likelihood of improvement in HE (meta-analysis 26311600)
✳️⬇️⬇️ICP from 37 to 13 on average (12602522) & resolution of CE on CT.
✳️average ⬇️ HE grade by 2 (West Haven)
✳️55% likelihood of improvement in HE (meta-analysis 26311600)

4.Effects on drug clearance:
Conventional dialysate didn’t remove diazepam but when switched to Albimin,level dropped👉🏻potential protein-bound drugs clearance.(22077243)
Most data w/ MARS is CCB/acetaminophen/mushroom poison.
How about Phenytoin/Valproate/BZD/Phenobarb toxicity?
Conventional dialysate didn’t remove diazepam but when switched to Albimin,level dropped👉🏻potential protein-bound drugs clearance.(22077243)
Most data w/ MARS is CCB/acetaminophen/mushroom poison.
How about Phenytoin/Valproate/BZD/Phenobarb toxicity?

Briefly,
❇️SPAD:unlike MARS, albumin is not recycled, discarded.
❇️Prometheus:Uses 250kDa filter👉🏻separate pt’s own albumin w/ toxins from 🩸👉🏻albumin rich plasma like solution passed through IE+AC👉🏻clear albumin-plasma remixed into🩸at the end of filter👉🏻through LFD👉🏻back to pt.
❇️SPAD:unlike MARS, albumin is not recycled, discarded.
❇️Prometheus:Uses 250kDa filter👉🏻separate pt’s own albumin w/ toxins from 🩸👉🏻albumin rich plasma like solution passed through IE+AC👉🏻clear albumin-plasma remixed into🩸at the end of filter👉🏻through LFD👉🏻back to pt.
Here’s one of our patient undergoing MARS for intractable pruritis..
This #emoryncctweetorial is only possible because @Capt_Ammonia has been pioneer in Neurocritical care fellow’s experience with MARS and transplant ICU @EmoryNeuroCrit , #RamSubbramanian
This #emoryncctweetorial is only possible because @Capt_Ammonia has been pioneer in Neurocritical care fellow’s experience with MARS and transplant ICU @EmoryNeuroCrit , #RamSubbramanian
So, if NH3 was the only culprit for HE, why not use just CRRT?
Yes, we can but NH3 clearance is UF rate dependent. Usual UF rate ~30ml/kg/hr is not enough to keep up w/ production of NH3. We need “high dose CRRT’- UF rate ~90ml/kg/hr.
Here’s the landmark study w/ data supporting.
Yes, we can but NH3 clearance is UF rate dependent. Usual UF rate ~30ml/kg/hr is not enough to keep up w/ production of NH3. We need “high dose CRRT’- UF rate ~90ml/kg/hr.
Here’s the landmark study w/ data supporting.

If you want to learn further about how CRRT works, follow this link to a great tweetorial by my co-fellow @EricLawson90
https://twitter.com/EricLawson90/status/1456382546636312580
@Capt_Ammonia @caseyalbin @CajalButterfly @ksuchdev @neurocritical @feras_akbik @JimmySuhMD @sigman_md @maness_caroline @mallyaa @JackieKraft4 @neuro_intensive @clhallmd @DetroitNeurons
• • •
Missing some Tweet in this thread? You can try to
force a refresh





