
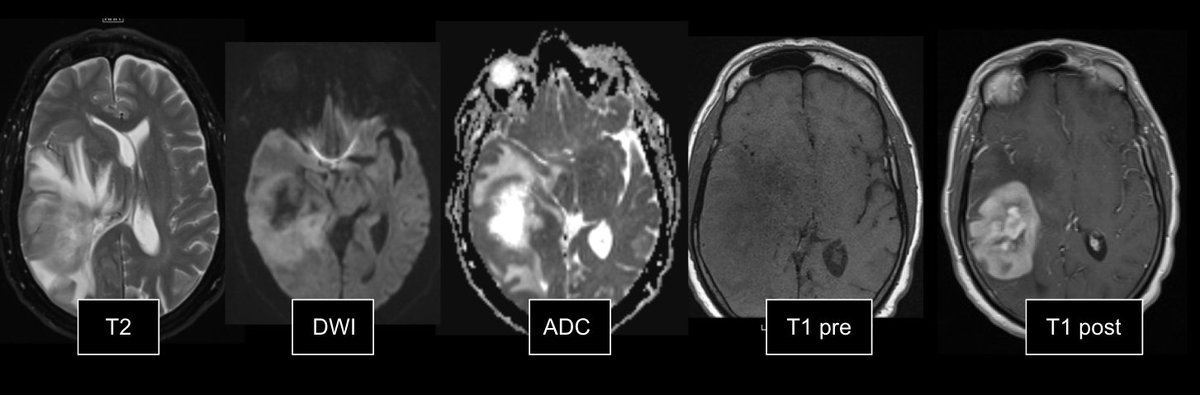
1/ 🧵Pt p/w headaches and 2 weeks of progressive left sided weakness. No history of immunosuppression. Open image of selected MRI brain w/ and w/o sequences ⬇️
#Medtwitter #neurotwitter #onctwitter #foam #foamncc #neurology #neuroonc
#Medtwitter #neurotwitter #onctwitter #foam #foamncc #neurology #neuroonc
2/ Biopsy can't be done for a few days. Would you Rx steroids before the biopsy?
3/ @AvrahamCooperMD had an illuminating #tweetorial regarding the “why” behind steroids for brain tumor vasogenic edema. tinyurl.com/4rtdsss6
🚨There is an exception to this practice!
Before biopsy when CNS lymphoma is suspected, we hold the steroids. BUT WHY?
🚨There is an exception to this practice!
Before biopsy when CNS lymphoma is suspected, we hold the steroids. BUT WHY?
4/ Goals for the scroll:
✅Why do we hold steroids prior to brain biopsy when CNS lymphoma is suspected?
✅ Discuss action of roids on lymphoid cells
✅Review the evidence of true roid effect on bx yield
✅Why do we hold steroids prior to brain biopsy when CNS lymphoma is suspected?
✅ Discuss action of roids on lymphoid cells
✅Review the evidence of true roid effect on bx yield
5/ Re the MRI -> CNS lymphoma suspected. Why?
💡Homo enhancement (het favors GBM, 🚫 enhancement ➡️ low-grade glioma)
💡 🚫thick enhancement of margins (which would be more c/w GBM, met, infx)
💡⬇️ADC in some areas (CNS lymphoma > GBM d/t ⬆️ cells and ⬆️ nucleus:cytoplasm)
💡Homo enhancement (het favors GBM, 🚫 enhancement ➡️ low-grade glioma)
💡 🚫thick enhancement of margins (which would be more c/w GBM, met, infx)
💡⬇️ADC in some areas (CNS lymphoma > GBM d/t ⬆️ cells and ⬆️ nucleus:cytoplasm)
6/ 🚨History is important too. No clinical risk factors/signs of infx or immunosupp (would favor infx process)
🦪Awesome CNS lymphoma ddx pearls @JohnJOkeefeMD: tinyurl.com/2p87j4ur & tinyurl.com/25knux3u
🦪Awesome CNS lymphoma ddx pearls @JohnJOkeefeMD: tinyurl.com/2p87j4ur & tinyurl.com/25knux3u
7/ Why do we hold steroids b4 bx of a tumor like this?
Classic teaching:🚫Roids held if suspect CNS lymphoma bc roids ➡️ acute lysis of lymphocytes ➡️ non dx biopsy
tinyurl.com/4jzt63vj and here tinyurl.com/4xny3pmk (also great for review of diff lymphomas in CNS)
Classic teaching:🚫Roids held if suspect CNS lymphoma bc roids ➡️ acute lysis of lymphocytes ➡️ non dx biopsy
tinyurl.com/4jzt63vj and here tinyurl.com/4xny3pmk (also great for review of diff lymphomas in CNS)
8/ And, other pathologies may be affected by roids: pubmed.ncbi.nlm.nih.gov/12221174/
Pathologies which may "vanish" w/ roids:
✅demyelinating disease
✅sarcoidosis
✅other tumors
Pathologies which may "vanish" w/ roids:
✅demyelinating disease
✅sarcoidosis
✅other tumors
9/ Lukas et al. tinyurl.com/4jzt63vj. Ex of non-dx vs. dx CNS lymphoma:
Thoughts? @CraigHorbinski #neuropath
Thoughts? @CraigHorbinski #neuropath

10/ But, why do steroids kill lymphomas (aka glucocorticoid -induced apoptosis of lymphoid cells)?
✅Glucocorticoids (GC) bind to GC receptor (GR) ➡️ goes to the nucleus where it modulates transcription of various genes and has a ton of other effects ➡️ cell death☠️🪦
✅Glucocorticoids (GC) bind to GC receptor (GR) ➡️ goes to the nucleus where it modulates transcription of various genes and has a ton of other effects ➡️ cell death☠️🪦
11/ GC do the following to lymphoid cells:
⬆️ in mitochon reactive ox species ➡️apoptosis
⬆️ tx of genes ➡️ proteins of apoptotic path
⬆️ destab of mitochondrial membrane ➡️☠️
⬆️ is cytosolic Ca ➡️ DNA fragmentation
⬆️K efflux → ⬆️ apoptosis
⬆️ in mitochon reactive ox species ➡️apoptosis
⬆️ tx of genes ➡️ proteins of apoptotic path
⬆️ destab of mitochondrial membrane ➡️☠️
⬆️ is cytosolic Ca ➡️ DNA fragmentation
⬆️K efflux → ⬆️ apoptosis

12/ The roid apoptotic effect: w/in min-hours! This makes roids great piece of tx regimens for heme maligs.
🚨some lymphoid cells have variable GR expression, GR mutations and mutations in other genes involved in apoptosis pathway ➡️ variable response to roids
🚨some lymphoid cells have variable GR expression, GR mutations and mutations in other genes involved in apoptosis pathway ➡️ variable response to roids
13/ 🧢Recap
✅ Roids = good for destroying lymphoma/leukemias
✅ So good at killing lymphoid cells = bad for biopsies
But... is this really true?
✅ Roids = good for destroying lymphoma/leukemias
✅ So good at killing lymphoid cells = bad for biopsies
But... is this really true?
14/ 🚨🚨Some more recent data suggests dx yield of bx in CNS lymphoma may not be that much diff in steroid vs. non-steroid tx pts
15/ Maybe bx yield not affected as much as we thought? ⁉️
1⃣tinyurl.com/55yps98f retro, PCNSL n=109 w/ 64% Rx steroids before bx → no stat sig diff in bx yield in roids vs. none
2⃣tinyurl.com/yuddvdam retro, PCNSL pts w/ no dec in bx yield in pts roids vs. no roids
1⃣tinyurl.com/55yps98f retro, PCNSL n=109 w/ 64% Rx steroids before bx → no stat sig diff in bx yield in roids vs. none
2⃣tinyurl.com/yuddvdam retro, PCNSL pts w/ no dec in bx yield in pts roids vs. no roids
16/ More
3⃣tinyurl.com/yckryhzp retro, n= 155; 135 w/ roids before bx (med duration 4 d); non-dx bx 10% in roid vs. no roid
4⃣tinyurl.com/mwm2x9ca only slight ⬇️ dx yield
5⃣tinyurl.com/ktkaefu4 no diff in bx yield roids <7 days vs. no roid; sig ⬇️ in yield roids >7 d
3⃣tinyurl.com/yckryhzp retro, n= 155; 135 w/ roids before bx (med duration 4 d); non-dx bx 10% in roid vs. no roid
4⃣tinyurl.com/mwm2x9ca only slight ⬇️ dx yield
5⃣tinyurl.com/ktkaefu4 no diff in bx yield roids <7 days vs. no roid; sig ⬇️ in yield roids >7 d
17/
These are all small studies, mostly retrospective. More data is needed.
But, why discord btw teaching of dec dx yield of roids pre-bx vs. more recent lit?
✅ Adv in imaging?
✅ Better surgical techniques?
These are all small studies, mostly retrospective. More data is needed.
But, why discord btw teaching of dec dx yield of roids pre-bx vs. more recent lit?
✅ Adv in imaging?
✅ Better surgical techniques?
18/ Round-up
✅ 🚫 roids B4 bx if ?CNS lymphoma
✅Roids ➡️ apoptosis lymph cells → ⬇️ dx yield
✅If clinical ⬇️ b4 bx → roids likely ok w/ multi-disc disc
✅If roids needed → get bx w/ in 1-2 dhttps://tinyurl.com/msmjjpj2
✅ New data: bx yld may be = in roid vs. non-roid pts
✅ 🚫 roids B4 bx if ?CNS lymphoma
✅Roids ➡️ apoptosis lymph cells → ⬇️ dx yield
✅If clinical ⬇️ b4 bx → roids likely ok w/ multi-disc disc
✅If roids needed → get bx w/ in 1-2 dhttps://tinyurl.com/msmjjpj2
✅ New data: bx yld may be = in roid vs. non-roid pts
19/ Discussion, feedback & practice pearls? 🦪🧋
@caseyalbin @EricLawson @JimmySuhMD @Tracey1milligan @mallyaa @JoshuaBudhu
@JayKinariwala @EKNduom @RebeccaFasanoMD @drdangayach @namorrismd @pouyeah @neuro_intensive @CajalButterfly @Capt_Ammonia
@caseyalbin @EricLawson @JimmySuhMD @Tracey1milligan @mallyaa @JoshuaBudhu
@JayKinariwala @EKNduom @RebeccaFasanoMD @drdangayach @namorrismd @pouyeah @neuro_intensive @CajalButterfly @Capt_Ammonia
• • •
Missing some Tweet in this thread? You can try to
force a refresh




