#AKIConsultSeries 👵➡️🏥 w necrotizing fasciitis s/p debridement. Significant 🩸 during surgery ➡️ intensive resuscitation (transfusions + crystalloid)
48 hrs later 💧📈 =+13 L, Edema +++, Hypoxemia, pleural effusion.
Now anuric unresponsive to high dose IV diuretics 1/10
48 hrs later 💧📈 =+13 L, Edema +++, Hypoxemia, pleural effusion.
Now anuric unresponsive to high dose IV diuretics 1/10

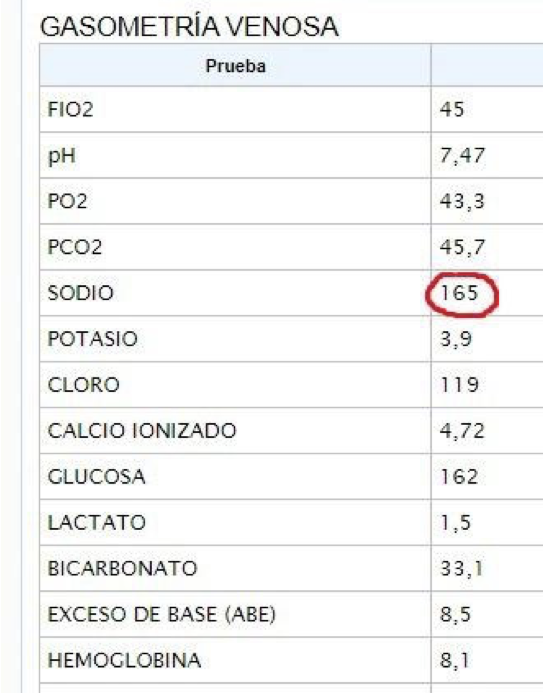
Cr 3.2, K 3.5, HCO3 25, Hb 8.9, WBC 26k, 95% PMN, Lactate 2.5
MAP 65 on NE (0.02 ucg/kg/min), HR 130, O2 sat 80-85 on 15 L NRB, RR 17 but w increased respiratory effort.🧠 drowsy, CRT >8 sec👇, JVP not elevated
Primary team consults for RRT initiation with ultrafiltration 2/10
MAP 65 on NE (0.02 ucg/kg/min), HR 130, O2 sat 80-85 on 15 L NRB, RR 17 but w increased respiratory effort.🧠 drowsy, CRT >8 sec👇, JVP not elevated
Primary team consults for RRT initiation with ultrafiltration 2/10
What would you do next? 3/10
#POCUS Very difficult acoustic window*
Collapsed IVC, Hyper-dynamic LV🫀 (++++), Pleural Effusion and 3-5 B Lines per zone bilaterally (not shown)
4/10
Collapsed IVC, Hyper-dynamic LV🫀 (++++), Pleural Effusion and 3-5 B Lines per zone bilaterally (not shown)
4/10
🚨🚨🚨 Warning 🚨🚨🚨
Dynamic Left Ventricular Outflow Tract Obstruction (DLVOTO) could be happening here!
💡Think of this when you see: Severe sepsis, ⬆️tachycardia, ⬇️ preload, kissing LV walls, mottled skin and ⬇️ pulse pressure
Be prepared!
journals.sagepub.com/doi/10.1177/03…
5/10
Dynamic Left Ventricular Outflow Tract Obstruction (DLVOTO) could be happening here!
💡Think of this when you see: Severe sepsis, ⬆️tachycardia, ⬇️ preload, kissing LV walls, mottled skin and ⬇️ pulse pressure
Be prepared!
journals.sagepub.com/doi/10.1177/03…
5/10
🚨DLVOTO can occur with significantly decreased LV filling volume
The inter-ventricular septum or the mitral valve might obstruct the LV outflow tract and cause a significant reduction in stroke volume
6/10
The inter-ventricular septum or the mitral valve might obstruct the LV outflow tract and cause a significant reduction in stroke volume
6/10

Remember obstruction causes an increase in velocity, so Doppler is essential for diagnosis
Even with a poor acoustic window, a simple CW Doppler through the LV Outflow Tract revealed a velocity of 4.3 m/s (gradient = 73 mmHg)!
This confirms DLVOTO!
7/10
Even with a poor acoustic window, a simple CW Doppler through the LV Outflow Tract revealed a velocity of 4.3 m/s (gradient = 73 mmHg)!
This confirms DLVOTO!
7/10


Treatment needs to be fast ⚡️
Maneuvers to increase LV volume: 1) Fluid Bolus, 2) Stop Inotropic Drugs, 3) Use non-inotropic vasopressor, 4) Carefully consider Beta-blocker
After fluid bolus and 🛑 NE, LVOT velocity decreased to less than 2!
8/10
Maneuvers to increase LV volume: 1) Fluid Bolus, 2) Stop Inotropic Drugs, 3) Use non-inotropic vasopressor, 4) Carefully consider Beta-blocker
After fluid bolus and 🛑 NE, LVOT velocity decreased to less than 2!
8/10

⚠️Fluid is not going to be a permanent fix because of expected extravasation!
A vasopressor with no inotropic/chronotropic properties should be initiated!
Vasopressin was given (0.08 UI)
Vitals improved, LVOT velocity remained < 2 m/s and UOP rose to >100 ml/hr!
9/10
A vasopressor with no inotropic/chronotropic properties should be initiated!
Vasopressin was given (0.08 UI)
Vitals improved, LVOT velocity remained < 2 m/s and UOP rose to >100 ml/hr!
9/10

DLVOTO is a catastrophic but potentially reversible condition. Be prepared!
If you want to learn more about DLVOTO here is another case of mine with a detailed explanation of the physiology of obstruction:
END/
If you want to learn more about DLVOTO here is another case of mine with a detailed explanation of the physiology of obstruction:
https://twitter.com/ArgaizR/status/1389010137772400641?s=20&t=r1TIq8qJtazdMVlwToNtRw
END/
• • •
Missing some Tweet in this thread? You can try to
force a refresh