
1/
Oh no! This patient is coming with heart failure exacerbation again. He is taking his diuretics but it seems they do not work. What can we do?
#DiureticResistanceMechanisms
#NephMadness #NephTwitter #MedTwitter
Oh no! This patient is coming with heart failure exacerbation again. He is taking his diuretics but it seems they do not work. What can we do?
#DiureticResistanceMechanisms
#NephMadness #NephTwitter #MedTwitter

2/
#DiureticResistance
Diuretic resistance is the failure to achieve euvolemia despite increasing doses or maximal tolerated diuretic therapy
#DiureticResistance
Diuretic resistance is the failure to achieve euvolemia despite increasing doses or maximal tolerated diuretic therapy

3/
What will be your first line to use to diurese a patient?
What will be your first line to use to diurese a patient?
4/
All of them may be used. However, loop diuretics are the most commonly used as they are the most potent.
A normal physiologic diuretic response to 40 mg of IV furosemide is 3-4 liters (L) of urine output containing 200-300 mmol of sodium in 3-4 hours
All of them may be used. However, loop diuretics are the most commonly used as they are the most potent.
A normal physiologic diuretic response to 40 mg of IV furosemide is 3-4 liters (L) of urine output containing 200-300 mmol of sodium in 3-4 hours

5/
What are the causes of #DiureticResistance?
Why is my diuretic not working?!!
⚡️Insufficient delivery of loop diuretics to the proximal tubule
⚡️Reabsorption of sodium at other nephron segments due to heightened sodium avidity aka “braking phenomenon”
What are the causes of #DiureticResistance?
Why is my diuretic not working?!!
⚡️Insufficient delivery of loop diuretics to the proximal tubule
⚡️Reabsorption of sodium at other nephron segments due to heightened sodium avidity aka “braking phenomenon”
6/
Causes for reduced delivery of Diuretic to PCT
1)Variable GI absorption
2)Low albumin for transporting the diuretic
3)Reduced kidney perfusion
4)Competition with other medications
5)Decreased amount of target receptors, due to renal damage
Causes for reduced delivery of Diuretic to PCT
1)Variable GI absorption
2)Low albumin for transporting the diuretic
3)Reduced kidney perfusion
4)Competition with other medications
5)Decreased amount of target receptors, due to renal damage

7/
Compensatory Na avidity or Braking Phenomenon is:
💧 Increased Na reabsorption at distal Sites
💧 A protective phenomenon.
Compensatory Na avidity or Braking Phenomenon is:
💧 Increased Na reabsorption at distal Sites
💧 A protective phenomenon.

8/
Compensatory Na avidity was thought to be the MAIN cause of diuretic resistance but this study suggests it may not be a dominant mechanism in ADHF compared to healthy controls.
DOI: 10.1093/eurheartj/ehab620
Compensatory Na avidity was thought to be the MAIN cause of diuretic resistance but this study suggests it may not be a dominant mechanism in ADHF compared to healthy controls.
DOI: 10.1093/eurheartj/ehab620

9/
Patients with advanced CHF & diuretic resistance are in a continuous sodium-avid state caused by
💧RAAS overactivation despite RAAS blockade
💧Aldosterone escape in CHF leading to ENaC & NDCBE-pendrin system activation in CD
💧Increased NaCl symporters through DCT hypertrophy
Patients with advanced CHF & diuretic resistance are in a continuous sodium-avid state caused by
💧RAAS overactivation despite RAAS blockade
💧Aldosterone escape in CHF leading to ENaC & NDCBE-pendrin system activation in CD
💧Increased NaCl symporters through DCT hypertrophy
10/
How can we distinguish between not enough delivery of diuretic to the PT vs heightened sodium avidity?
1) Check spot urine collected 2H after giving a diuretic to check natriuresis
2) Fancy lab? Check FeLi. It will ↑. Lithium will not be reabsorbed in the distal nephron
How can we distinguish between not enough delivery of diuretic to the PT vs heightened sodium avidity?
1) Check spot urine collected 2H after giving a diuretic to check natriuresis
2) Fancy lab? Check FeLi. It will ↑. Lithium will not be reabsorbed in the distal nephron
11/
☑️Once we have assessed causes of diuretic resistance, let's check if the patient is truly de-congested. 💧
Weight and fluid output are the most commonly used measurements for monitoring diuretic response. However, nowadays we have more objective tools.
☑️Once we have assessed causes of diuretic resistance, let's check if the patient is truly de-congested. 💧
Weight and fluid output are the most commonly used measurements for monitoring diuretic response. However, nowadays we have more objective tools.
12/
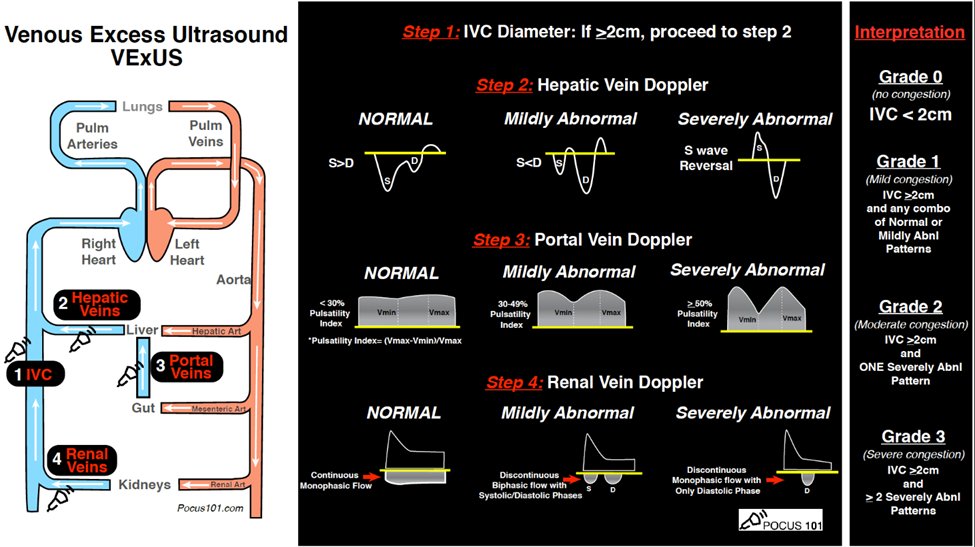
Want to be more precise? Let’s try Excess Ultrasound Score (VExUS): A tool to assess venous congestion.
Follow the video link to learn more: nephropocus.com/2020/12/12/wha…
Want to be more precise? Let’s try Excess Ultrasound Score (VExUS): A tool to assess venous congestion.
Follow the video link to learn more: nephropocus.com/2020/12/12/wha…
13/
That's all for now folks.
Keep posted to hear about how to manage diuretic resistance.
Read more about this here:
ajkdblog.org/2022/03/01/nep….
That's all for now folks.
Keep posted to hear about how to manage diuretic resistance.
Read more about this here:
ajkdblog.org/2022/03/01/nep….
14/
Thanks to #NSMC #NephMadness #NephTwitter #MedTwitter
@swastithinks @amyaimei @Nephro_sparks @docanjuyadav @menonshina @Elena_Cervants @JMTeakell @nephromythri
Thanks to #NSMC #NephMadness #NephTwitter #MedTwitter
@swastithinks @amyaimei @Nephro_sparks @docanjuyadav @menonshina @Elena_Cervants @JMTeakell @nephromythri

Follow #Pod2k22 for ongoing
@NephMadness
tweetorials!
@kidneymo
@Hmzrage
@kidneyrachael
@bilalksheikh
@merlomar2109
@anandthedoc
@hemoncfellow
@nsmcinternship
@rachhung
@WilliamVasEsp
@NephMadness
tweetorials!
@kidneymo
@Hmzrage
@kidneyrachael
@bilalksheikh
@merlomar2109
@anandthedoc
@hemoncfellow
@nsmcinternship
@rachhung
@WilliamVasEsp
• • •
Missing some Tweet in this thread? You can try to
force a refresh


