🎖 #ACC_AHA_HFSA #HF Guidelines are out
Short Tweetorial
🍀 Congrats to the authors for the huge effort : 108 pgs covering multiple aspects including #CardiacAmyloid
@ShelleyZieroth @hvanspall @carlosguizars @ValleAlfonso @JavedButler1 @gcfmd @JJheart_doc
rb.gy/ocnlb7
Short Tweetorial
🍀 Congrats to the authors for the huge effort : 108 pgs covering multiple aspects including #CardiacAmyloid
@ShelleyZieroth @hvanspall @carlosguizars @ValleAlfonso @JavedButler1 @gcfmd @JJheart_doc
rb.gy/ocnlb7


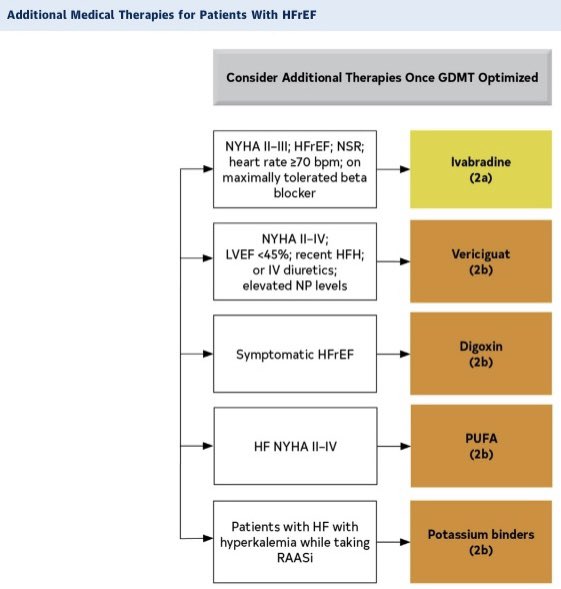
1️⃣ #HFrEF tx
✅ Pros: Clear 4 pillar 1st line 1 day ( No wait)
❌ Cons: NYHA is not fixed very changeable : Better using Hypotension (SBP<100 mmHg) as choice criteria for ACE/ARB vs ARNI
❌ Cons: After 1 + 1/2 year from #GALACTIC_HF Omecamtiv Mecarbil still not in GD
✅ Pros: Clear 4 pillar 1st line 1 day ( No wait)
❌ Cons: NYHA is not fixed very changeable : Better using Hypotension (SBP<100 mmHg) as choice criteria for ACE/ARB vs ARNI
❌ Cons: After 1 + 1/2 year from #GALACTIC_HF Omecamtiv Mecarbil still not in GD

2️⃣ #HFmrEF
✅ Pros: Concur with HFmrEF recom.
⭕️ Probably a 2a in this class for #ARNI is more EBM
@DrNasrien @dranulala @robmentz @MicheleSenni @DrDEliaEmilia @gbiondizoccai @torresviera @JavierdeJuan1 @global_meded @Filippatos @YuriLopatin1
#ACC22
✅ Pros: Concur with HFmrEF recom.
⭕️ Probably a 2a in this class for #ARNI is more EBM
@DrNasrien @dranulala @robmentz @MicheleSenni @DrDEliaEmilia @gbiondizoccai @torresviera @JavierdeJuan1 @global_meded @Filippatos @YuriLopatin1
#ACC22

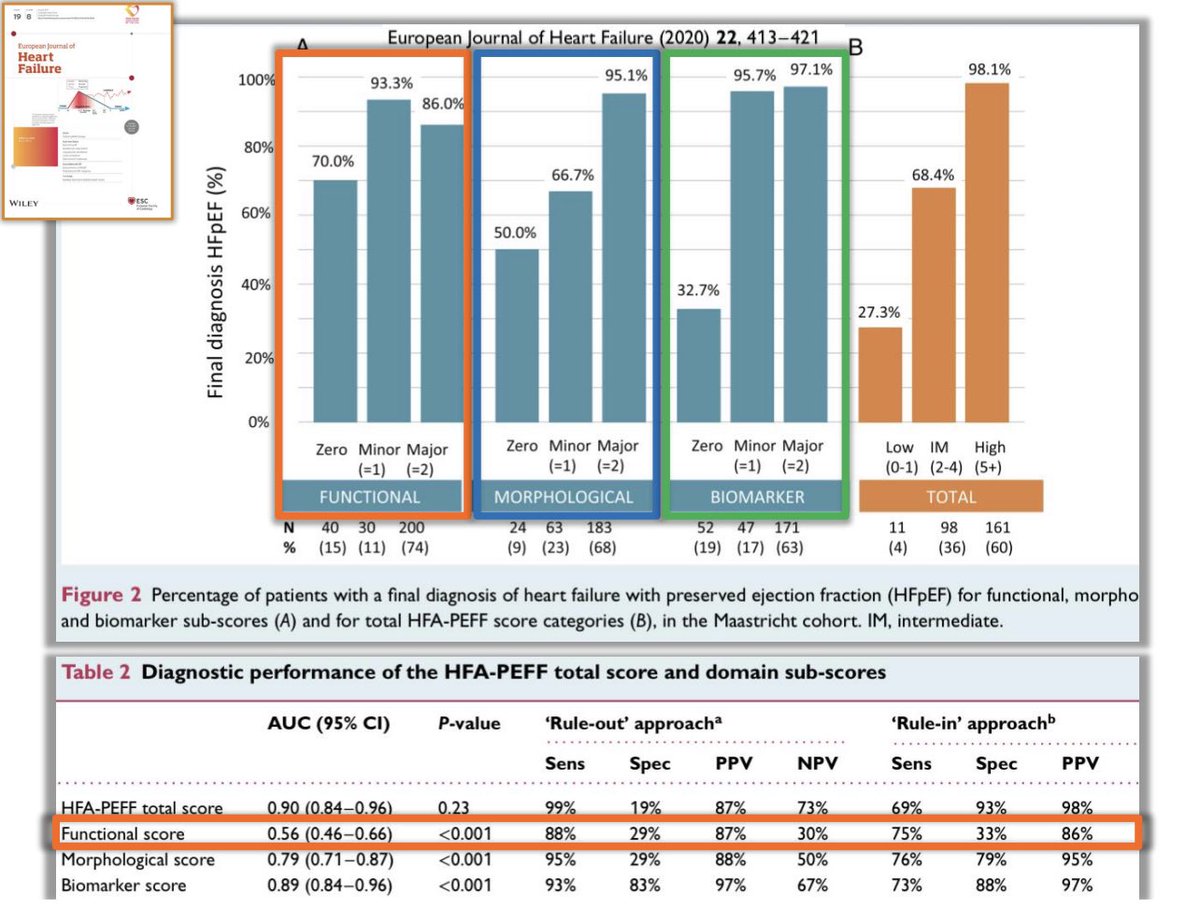
3️⃣ #HFpEF
✅ #SGLT2i in
❌ Cons: Diuretics Class I (No RCT, This are GD on #HF not on #Hypertension) very questionable
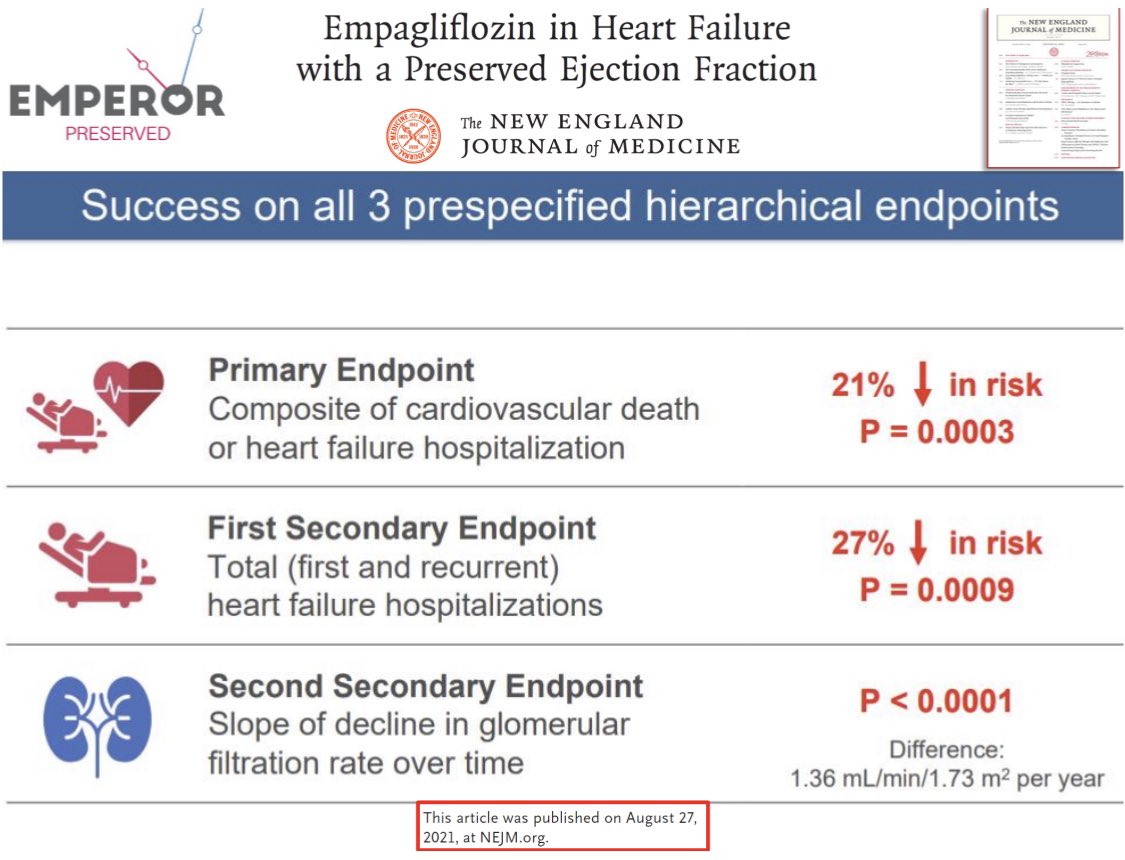
❌ Especially when #EMPEROR_PRESERVED (~ 6000 pts RCT) positive & only 2a?
Because not significant on #CV_Death? 🥶
Someone is missing the point in #HFpEF
✅ #SGLT2i in
❌ Cons: Diuretics Class I (No RCT, This are GD on #HF not on #Hypertension) very questionable
❌ Especially when #EMPEROR_PRESERVED (~ 6000 pts RCT) positive & only 2a?
Because not significant on #CV_Death? 🥶
Someone is missing the point in #HFpEF


4️⃣ A major paradigm shift should be done in #HFpEF
🍀 These pts are very old at diagnosis (76 mean age in 🇮🇹 & in all registries over the last 15-20 yrs)
🍀 Mean expectancy of life from diagnosis to death in mean 6-7 year
🎯 Our target is ⬆️ #QoL & ⬇️ #HHF
@ShelleyZieroth
🍀 These pts are very old at diagnosis (76 mean age in 🇮🇹 & in all registries over the last 15-20 yrs)
🍀 Mean expectancy of life from diagnosis to death in mean 6-7 year
🎯 Our target is ⬆️ #QoL & ⬇️ #HHF
@ShelleyZieroth



5️⃣ Final
🔥 Rita Levi Montalcini : Nobel Prize 1986 ✅ “Better adding life to days than days to life”
👌 Perfect for #HFpEF
🍀#SGLT2i Class I
👉 “Science go faster than guidelines”
🍀 next year new #GD
🍀 My hope high-time for TransAtlantic GD ACC_AHA_HFSA/ ESC_HFA
@DLBHATTMD
🔥 Rita Levi Montalcini : Nobel Prize 1986 ✅ “Better adding life to days than days to life”
👌 Perfect for #HFpEF
🍀#SGLT2i Class I
👉 “Science go faster than guidelines”
🍀 next year new #GD
🍀 My hope high-time for TransAtlantic GD ACC_AHA_HFSA/ ESC_HFA
@DLBHATTMD




• • •
Missing some Tweet in this thread? You can try to
force a refresh