
Apologies for confusion. Here is this morning's proceedings from the tribunal of Dr. Michael Webberley. This afternoon's live tweeting will appear here.
https://twitter.com/tribunaltweets/status/1511991035831988226
Now restarting after the lunch break.
SJ: Simon Jackson, QC for GMC
AK: Alanna Kieran, expert witness
RD: Ryan Donoghoue, counsel for GMC
Chair: chair of the tribunal panel
Panel: other members of panel
SJ: Simon Jackson, QC for GMC
AK: Alanna Kieran, expert witness
RD: Ryan Donoghoue, counsel for GMC
Chair: chair of the tribunal panel
Panel: other members of panel
SJ: discussion of documents regarding Patient W and the statement that there are no medical records available. There apparently are some records, but were not made available until after disclosure was finished.
Chair: documents will be made available.
Chair: documents will be made available.
SJ: Moving on to Patient V. Message to support at 'MyWebDoctor' with history of patient, referencing issue of patient's identity. Written by parent on behalf of V. Desperate to get on hormone blockers as soon as possible, mood shifting etc. Patient just under 10 years of age.
SJ; see a reply from MW to mother, 'very happy to help you (why do they have to go through puberty so young?), there is a big process to go through, who will inject the hormones, is your GP on board?, can the practice nurse do the injections or teach you'
SJ: what is your impression AK on this?
AK: mum's history is comprehensive and clear there is distress. But it is complete inappropriate to start out with the assumption that puberty blockers will be prescribed, negates the purpose of diagnosis and assessment.
AK: mum's history is comprehensive and clear there is distress. But it is complete inappropriate to start out with the assumption that puberty blockers will be prescribed, negates the purpose of diagnosis and assessment.
SJ: now in AK's report. 2 professionals involved in V's care, both counsellors. Can you set out what you would have expected to happen?
AK: MDT assessment of child, family, expert in child development as well as GI, plus medical professional who is going to possibly prescribe.
AK: MDT assessment of child, family, expert in child development as well as GI, plus medical professional who is going to possibly prescribe.
SJ: what should be the sequence of contact with GP, other professionals and blood tests before assessment.
AK: we would engage the GP from the beginning following the shared care guidelines, endocrinologist would initiate and possibly GP would take over after 3-6 months.
AK: we would engage the GP from the beginning following the shared care guidelines, endocrinologist would initiate and possibly GP would take over after 3-6 months.
SJ: Do they same starting points exist with this patient, that they should be followed.
AK: the child is 9 and the same considerations apply, how best to have a 9 year old participate in the assessment. The child didn't speak during the assessment only the parents.
AK: the child is 9 and the same considerations apply, how best to have a 9 year old participate in the assessment. The child didn't speak during the assessment only the parents.
AK: It is important that an expert with experience in dealing with children is engaged in the discussion, can build trust, encourage communication with the child.
SJ: Referring to written questionnaires and referring to get blood tests done. what is the relevance of blood tests.
SJ: Referring to written questionnaires and referring to get blood tests done. what is the relevance of blood tests.
AK: we wouldn't do blood tests until we were ready to prescribe so after assessment, and we would do it prior to agreeing that treatment could commence.
SJ: Referring to document, 'Gender Identity under the Age of 16'. Questions were read to 9 year old child by mother.
SJ: Referring to document, 'Gender Identity under the Age of 16'. Questions were read to 9 year old child by mother.
SJ: And if not applicable did not read them the questions. What do you think of that.
AK: The questions are described as under 16 but not appropriate for 9 year old. Reading the answers there is no way of knowing what the child thinks. And some of the questions mum deemed
AK: The questions are described as under 16 but not appropriate for 9 year old. Reading the answers there is no way of knowing what the child thinks. And some of the questions mum deemed
AK: 'not applicable' we would certainly explore those areas with a 9 year old. Needs an experienced clinician to explore with the child. All of this through the lens of the mother.
SJ: GenderGP 'questionnaire answered fully', please send link for info gathering session.
SJ: GenderGP 'questionnaire answered fully', please send link for info gathering session.
SJ: Given that mother decided some questions were not relevant, how could counsellor deem questions fully answered?
AK: they weren't fully answered and this is the difficulty.
SJ: From records 'Responses reviewed by MDT, no issues raised' entry by MW.
AK: they weren't fully answered and this is the difficulty.
SJ: From records 'Responses reviewed by MDT, no issues raised' entry by MW.
SJ: is this an actual MDT?
AK: it should have been described as responses from a single member of the MDT, not the actual MDT.
SJ: is MW's role a proactive role or a reactive role?
AK: others should gather the info, but then discussed and agreed all together.
AK: it should have been described as responses from a single member of the MDT, not the actual MDT.
SJ: is MW's role a proactive role or a reactive role?
AK: others should gather the info, but then discussed and agreed all together.
SJ: on the 'no concerns raised', is this adequate?
AK: many responses that I would like to explore further with the child, not to mention the questions that were not answered. I would like to encourage further exploration and differences between gender roles and gender identity.
AK: many responses that I would like to explore further with the child, not to mention the questions that were not answered. I would like to encourage further exploration and differences between gender roles and gender identity.
SJ: counsellors and psychogender therapist, are you familiar with this?
AK: it's not a term that I recognise or I would use myself.
SJ: reads out elements of the report.
AK: first, they are inaccurately reporting the age of the child who is 9, not 12.
AK: it's not a term that I recognise or I would use myself.
SJ: reads out elements of the report.
AK: first, they are inaccurately reporting the age of the child who is 9, not 12.
AK: areas requiring further exploration: child was very shy and did not speak, mother answered all the questions. I would like to engage directly with the child to understand their feelings. No signs of mental health assessment, for example looking for autism spectrum disorder.
AK: and no discussion of fertility.
SJ: the phrase 'no reason not to prescribe, no reason not to help them'
AK: they haven't actually said how the patient meets the diagnostic criteria. It's not about being helpful or no, it's about meeting the diagnostic criteria.
SJ: the phrase 'no reason not to prescribe, no reason not to help them'
AK: they haven't actually said how the patient meets the diagnostic criteria. It's not about being helpful or no, it's about meeting the diagnostic criteria.
SJ: reads out parts of the standard letter, will your GP help, do you need counselling,
AK: the statement 'we have completed the administrative side' appears as a tickbox exercise rather than a chance for the child to explore in a therapeutic space.
AK: the statement 'we have completed the administrative side' appears as a tickbox exercise rather than a chance for the child to explore in a therapeutic space.
AK: also, the implication that counselling is the exception or shouldn't be needed, not the norm. Finally, asking for the detailed summary is an attempt to document the patients understanding. It is not sufficient, it fails at that.
SJ: now an email to Patient V & Mother, asking about surgery and stage of puberty. Where does that fit in, is it appropriate.
AK: it is appropriate, blockers are prescribed at Tanner stage 2. That's appropriate but usually undertaken by the paediatric endocrinologist.
AK: it is appropriate, blockers are prescribed at Tanner stage 2. That's appropriate but usually undertaken by the paediatric endocrinologist.
SJ: then a reply from the mother, doing the assessment of puberty.
AK: I can only relate my experience, our endocrinologist would absolutely demand to do the exam themselves.
SJ: Quoting ME email I'm thinking about someone else to get your second assessment done.
AK: I can only relate my experience, our endocrinologist would absolutely demand to do the exam themselves.
SJ: Quoting ME email I'm thinking about someone else to get your second assessment done.
SJ: an appropriate step?
AK: yes an appropriate step.
SJ: problems with email, also your paediatrician has expressed concerns, I will be making the final decisions, we will have our child psychologist undertake the second assessment.
AK: yes an appropriate step.
SJ: problems with email, also your paediatrician has expressed concerns, I will be making the final decisions, we will have our child psychologist undertake the second assessment.
SJ: what is the paediatricians concern?
AK: that the child was going on blockers, after no real period of assessment and via a private doctor and not the NHS.
SJ: now referring to consent form that combines puberty blockers and cross sex hormones.
AK: that the child was going on blockers, after no real period of assessment and via a private doctor and not the NHS.
SJ: now referring to consent form that combines puberty blockers and cross sex hormones.
SJ: is that appropriate?
AK: it is confusing especially for a 9 year old child. What side effect applies to which. It also implies that its a single step approach blockers plus x sex hormones.
AK: it is confusing especially for a 9 year old child. What side effect applies to which. It also implies that its a single step approach blockers plus x sex hormones.
SJ: now quoting MW notes from Skype assessment. Dangerous to not proceed. Recommends that child goes on blockers. What are your comments.
AK: the comments around danger and mental health problems are common in gender distressed children. But that's general not specific to
AK: the comments around danger and mental health problems are common in gender distressed children. But that's general not specific to
AK: this patient. Doesn't speak to this child's mental health. Says 'buy time and make further assessments'. But then no further assessments are actually offered or carried out. Treatment should be part of a care plan, showing how it will help,
AK: and what further steps might be contemplated.
SJ: now discussing MW comments on the need for the physical examination of the child and the psychological examination and assessment of the child. Does the Skype consult meet either of these criteria?
SJ: now discussing MW comments on the need for the physical examination of the child and the psychological examination and assessment of the child. Does the Skype consult meet either of these criteria?
AK: no it does not satisfy those criteria. It may provide information to the child, moving towards informed consent. But it doesn't address the physical examination of puberty or mental health assessment by a child psychologist.
SJ: could MW carry out mental health assessment
SJ: could MW carry out mental health assessment
AK: no I don't imagine he's competent to do that.
Chair: statement in document 'if puberty is allowed to progress further there is a very real danger of self harm or mental health issues'. Is there any evidence of these risks in the patient's records?
AK: I saw nothing that would indicate self harm or mental health problem
AK: I saw nothing that would indicate self harm or mental health problem
AK: this patient had many protective factors to mitigate the general harm.
SJ: in the context of a referral to a paediatric endocrinologist, is it about the time to prescribe.
AK: yes it is important that children have some 'taste' of puberty, hence Tanner Stage 2,
SJ: in the context of a referral to a paediatric endocrinologist, is it about the time to prescribe.
AK: yes it is important that children have some 'taste' of puberty, hence Tanner Stage 2,
AK: the child may find that puberty is not as distressing as they feared. Also, if puberty hasn't started it gives time for exploration and discussion and to get to know the child.
SJ: A prescription is written that same day as the Skype consultation.
SJ: A prescription is written that same day as the Skype consultation.
SJ: prescription written 2 minutes after the documentation of the skype consultation.
AK: Yes.
SJ: now moving on to witness statement from Patient V's mother.
AK: Yes.
SJ: now moving on to witness statement from Patient V's mother.
SJ: mother 'I made contact with MW on 17 May, provided details, explanation, responded same day, happy to help, biggest question, who was going to administer the blockers. Reference to more than one GP' On 16 July, 20 minute Skype meeting with mother and Patient V.
SJ: 10 minutes of discussion with V present, when MW asked about how V feels about gender etc. Then child left the room. What's your opinion on the adequacy of that?
AK: it is very inadequate, it takes time to establish rapport and trust with a 9 year old child.
AK: it is very inadequate, it takes time to establish rapport and trust with a 9 year old child.
AK: not possible in 10 minutes.
SJ: how long does that rapport and trust take in your experience?
AK: we would have probably 6 assessment appointments, some without the parents present after the first few appointments. We would combine information about treatments with
SJ: how long does that rapport and trust take in your experience?
AK: we would have probably 6 assessment appointments, some without the parents present after the first few appointments. We would combine information about treatments with
AK: the assessment. Then in subsequent assessments we could see what their level of understanding is, how much information they retain, are their expectations of transition realistic?
SJ: now going back to report, adequacy of ASD assessment.
SJ: now going back to report, adequacy of ASD assessment.
AK: we always do specific autism spectrum disorder (ASD) screening, even if already diagnosed. It is not to imply that ASD children cannot access blockers, but it is important for communication especially.
SJ: your views on the responsibility of the prescriber
AK: the responsibility lies with the prescriber, to ensure that the diagnosis is met, that the treatment is indicated and has opportunity to succeed.
SJ: why is the diagnostic assessment important?
AK: the responsibility lies with the prescriber, to ensure that the diagnosis is met, that the treatment is indicated and has opportunity to succeed.
SJ: why is the diagnostic assessment important?
AK: there are set guidelines for how a diagnosis is made, documented etc. These are important for the treatment plan.
SJ: what are your expectations on exploration of other treatments.
AK: I would go with the WPATH guidelines, extensive exploration of identity.
SJ: what are your expectations on exploration of other treatments.
AK: I would go with the WPATH guidelines, extensive exploration of identity.
SJ: why is fertility important
AK: we would explore this, even with a very young child, to the extent they are able to imagine their future. This is where you can see they may have very unrealistic expectations about their future fertility after transition.
AK: we would explore this, even with a very young child, to the extent they are able to imagine their future. This is where you can see they may have very unrealistic expectations about their future fertility after transition.
SJ: now on to capacity and consent. Did Patient V undergo full psychological counselling and assessment?
AK: no that did not happen
SJ: regular counselling sessions?
AK: no, did not happen.
SJ: reading out various parts of consent form, signature confirms
AK: no that did not happen
SJ: regular counselling sessions?
AK: no, did not happen.
SJ: reading out various parts of consent form, signature confirms
SJ: my doctor has explained risks, side effects, etc. Reading all that after a 10 minute conversation with a child, what's your assessment, did the child understand what they were signing up to?
AK: no it is wholly inadequate. Much is not relevant and
AK: no it is wholly inadequate. Much is not relevant and
AK: much too much detail, they could not possibly have understood what they were signing up to.
SJ: MW says Gillick competent, can you see that?
AK: it is not clear, its implied it was determined during the Skype consult.
SJ: how should it be done:
SJ: MW says Gillick competent, can you see that?
AK: it is not clear, its implied it was determined during the Skype consult.
SJ: how should it be done:
AK: we would have a discussion with the child, together write down all the psycho social documentation. Then they would go the endocrinologist and go through a document on the physical side effects. We document that we have gone through all of the effects with the child.
SJ: you say no attempt by MW to assess the impact of the blockers. What do you mean?
AK: blockers are given to reduce to distress - is distressed reduced? Are there any side effects present? Needs to be a direct review with the child. What is the thinking about hormones?
AK: blockers are given to reduce to distress - is distressed reduced? Are there any side effects present? Needs to be a direct review with the child. What is the thinking about hormones?
Breaking now for 15 minutes.
Resuming now.
SJ: going back to Patient S. Born in 1999, contacted GenderGP at 17 years old. Noted in AKs report, S had been known to CAMHS since age 13. One off assessment session, unsurprising insufficient information gathered to make diagnosis. Now referring to witness statement
SJ: of consultant psychiatrist of Patient S. Reads out from statement, 'got fax letter from MW at GenderGP in August, first communication from them. Tried to call MW a few times, unsuccessful.'. Now a letter sent by CAMHS specialist psychiatrist, to patient
SJ: discussing blood tests, mentioned letter from MW.
SJ: Now reading letter - specialist to MW, says won't be able to prescribe for Patient S. Will discharge to own GP once referred for hormones' Why is it important to have direct contact with others who have worked with S?
SJ: Now reading letter - specialist to MW, says won't be able to prescribe for Patient S. Will discharge to own GP once referred for hormones' Why is it important to have direct contact with others who have worked with S?
AK: Patient S has ASD, thus communication difficulty, important to speak with others who have known the patient. Find out what other challenges or concerns there may be. MW didn't take the time to liaise, didn't return the call from CAMHS doctor.
SJ: do you understand the guidelines for a medical practitioner to work together?
AK: I understand the WPATH guidelines, but not the medical requirements.
Now questions from the panel.
AK: I understand the WPATH guidelines, but not the medical requirements.
Now questions from the panel.
Panel: I'm a lay member, so possibly quite simple questions. Going back to Patient V, on fertility. The questionnaire seems to deal with this. Then we see the asterisk. Means it has been completed by mother. Child has said, 'never wanted a baby in the tummy'.
Panel: Is this an example of 'answers given through the prism of the mother'.
AK: yes, it's a closed question and answer. Not casting doubt on mum's recollection but closes out the possibility of an exchange and exploration.
Panel: is this a topic area that would be explored?
AK: yes, it's a closed question and answer. Not casting doubt on mum's recollection but closes out the possibility of an exchange and exploration.
Panel: is this a topic area that would be explored?
AK:Yes, it would be explored in subsequent sessions. It might be consistently expressed or their views might changing or variable.
Panel: in terms of adequacy, is this an adequate interaction or understanding of Patient S's fertility?
AK: No, not adequate.
Panel: in terms of adequacy, is this an adequate interaction or understanding of Patient S's fertility?
AK: No, not adequate.
Panel: more understanding of Tanner Stage 2. Has it been arrived at? Does it need a physical examination or are questions adequate? What about blood tests?
AK: blood tests - ask my medical colleagues. But there would have been a physical examination.
AK: blood tests - ask my medical colleagues. But there would have been a physical examination.
AK: examine the chest, the genitals, the amount of body hair.
Panel: necessary independent examination?
AK: Yes, and also to address general physical health and bone density assessment.
Panel: age of onset of puberty? Age is a factor
Panel: necessary independent examination?
AK: Yes, and also to address general physical health and bone density assessment.
Panel: age of onset of puberty? Age is a factor
Panel: but not the only factor.
AK: yes, relevant but variable and physical examination relevant.
Panel: what is the youngest child you've seen.
AK: in the beginning we sent all 12 -15 to the Tavistock. Now I think the youngest we've treated is 12.
AK: yes, relevant but variable and physical examination relevant.
Panel: what is the youngest child you've seen.
AK: in the beginning we sent all 12 -15 to the Tavistock. Now I think the youngest we've treated is 12.
Handing back to chair.
Chair: going back to the age of the child. There is no specific age cutoff at which blockers are indicated. But puberty blockers are appropriate at Tanner Stage 2.
AK: not a specific age in professional guidance. It is trying to balance.
Chair: going back to the age of the child. There is no specific age cutoff at which blockers are indicated. But puberty blockers are appropriate at Tanner Stage 2.
AK: not a specific age in professional guidance. It is trying to balance.
AK: the level of the child's distress with allowing some experience of puberty. If a high level of distress is present, then there is more risk. The onus is on us as clinicians to use the time to explore the issues. Unfortunately,
Gender GP patients, the prescription of blockers was the end of treatment and no exploration of the mental health or gender dysphoria.
Chair: Young patients, T, V; either they had capacity and were Gillick competent or they weren't. You said,
Chair: Young patients, T, V; either they had capacity and were Gillick competent or they weren't. You said,
Chair: before the age of 16, parental consent. After 16, child's consent with parental consent desired. You would never override the child's consent. Could the parents and the MDT make the decision where the child has not consented?
AK: not within my experience. But we had a younger child where we were concerned that they didn't actually understand the consequences or have the knowledge. Can't imagine the circumstances where we proceed if the child did not want to have treatment.
Chair: can you imagine going forward with treatment if the child couldn't consent if the parents did consent?
AK: I can't imagine we would do that. We might wait until the child was consequences.
Chair: it is a very exceptional case that the child was prescribed blockers,
AK: I can't imagine we would do that. We might wait until the child was consequences.
Chair: it is a very exceptional case that the child was prescribed blockers,
Chair: if the child was not Gillick competent.
AK: it would be exceptional.
Chair: identified that fertility is an important issue to be discussed. If puberty blockers are wholly reversible, the decision as to blockers vs hormone therapy
AK: it would be exceptional.
Chair: identified that fertility is an important issue to be discussed. If puberty blockers are wholly reversible, the decision as to blockers vs hormone therapy
Chair: is a two step process. Why is it necessary to address this until cross sex hormones are prescribed.
AK: Good question. For children AMAB, they have to come off blockers to produce sperm to preserve fertility.
So they still have to go through the distress, etc.
AK: Good question. For children AMAB, they have to come off blockers to produce sperm to preserve fertility.
So they still have to go through the distress, etc.
AK: for children AFAB, they can go through fertility preservation but the wait for it is very long. So we like to deal with those issues early on to get them on the waiting lists.
AK: also, having these discussions informs us about the young person's ability to think about
AK: also, having these discussions informs us about the young person's ability to think about
AK: the future. It's a good insight into their mental development and their ability to envisage the future.
Chair: you always (only) in your service take referrals from CAMHS.
AK: Yes we take referrals from CAMHS.
Chair: Then referred to you, waiting time for both.
Chair: you always (only) in your service take referrals from CAMHS.
AK: Yes we take referrals from CAMHS.
Chair: Then referred to you, waiting time for both.
Chair: then once seen, a minimum 3 month assessment, could be 6 month assessment.
AK: yes, plus delays in referral to endocrinologist.
Chair: with all this waiting some children may be waiting so long, by the time they get the puberty blockers, it may be too late.
AK: yes, plus delays in referral to endocrinologist.
Chair: with all this waiting some children may be waiting so long, by the time they get the puberty blockers, it may be too late.
AK: yes, this is a problem. But this is not a reason to shortcut the assessment process. You could substantially shorten the time for the assessment in private practice. Quicker but still in depth.
AK: access via CAMHS is designed to support the young person
AK: access via CAMHS is designed to support the young person
AK: all through out the process. They have a local therapist that can support them through CAMHS.
Chair: it might be argued that if you have a child suffering gender dysphoria, if blockers are reversible, isn't it better that they get treatment quickly,
Chair: it might be argued that if you have a child suffering gender dysphoria, if blockers are reversible, isn't it better that they get treatment quickly,
Chair: not expressing that point of view, inviting you to comment.
AK: First, I referred earlier to diagnosis overshadowing, the idea that the problem can only be dealt with through medical intervention. The risk of rushing to prescribe a hormone blocker,
AK: First, I referred earlier to diagnosis overshadowing, the idea that the problem can only be dealt with through medical intervention. The risk of rushing to prescribe a hormone blocker,
AK: is that you miss all the other things may be going on in the child's life. And the chance to help them with those issues. The other problem is that once a child goes onto blockers they are very likely to progress to cross sex hormones. We don't understand why that is.
AK: we are trying always to balance the risk of acting vs the risk of not acting. Do we know the child well enough to set them on a medical pathway that is very likely to progress to cross sex hormones?
Chair: now talking about those named MW's MDT. You said you did not know what a 'gender psychotherapist' was, not a job description you were familiar with. You can also see 'BACPS', are you familiar with that?
AK: yes, body for counsellors.
Chair: referring to members of MDT and WPATH guidelines. Sets out minimum credentials for those working in the area, mental health professionals, description of the competency areas. Other health professionals with training may conduct
Chair: referring to members of MDT and WPATH guidelines. Sets out minimum credentials for those working in the area, mental health professionals, description of the competency areas. Other health professionals with training may conduct
Chair: assessments, particularly as part of an MDT. Referring back to the list of members: can you tell if they meet the criteria as mental health professionals or health professionals.
AK: no, I cannot comment.
AK: no, I cannot comment.
Panel: Going back to Tanner Stage 2. Previous expert, said 12. You've said no one younger than age 12. Previous expert said the child should experience Tanner Stage 2, not 'hit stage 2, now blockers'. Do you agree?
AK: I would see that more as an individual question.
AK: I would see that more as an individual question.
AK: we tend to see children once they've started puberty because there really isn't distress before that point. I would consider each child's presentation individually, both physical and mental, before making a recommendation.
AK: children can change a great deal between primary school and secondary school, much development occurs.
Panel: would you still take into account the Tanner stage even if there's the distress?
AK: if there are no changes, why the distress? We need to explore why.
Panel: would you still take into account the Tanner stage even if there's the distress?
AK: if there are no changes, why the distress? We need to explore why.
Panel: would you involve the endocrinologist ?
AK: possibly to confirm state of puberty but not normally until we are ready to make or consider a referral.
Panel: now going back to composition of MDT. Is it adequate or normal?
AK: possibly to confirm state of puberty but not normally until we are ready to make or consider a referral.
Panel: now going back to composition of MDT. Is it adequate or normal?
AK: Its' hard to say, we have paediatric endocrinologist, specialist nurses, family therapist, etc. They don't seem to have the psychiatrist angle. We feel our team is well rounded and well resourced.
Panel: what about the absence of the paediatric endocrinologist?
Panel: what about the absence of the paediatric endocrinologist?
AK: it feels very important that we have a paediatrician with the endocrine specialism made a big difference for us. But maybe the medical experts are better qualified to judge.
Panel: what about the absence of psychiatric support?
Panel: what about the absence of psychiatric support?
AK: I don't see that the psychologist can supply the necessary expertise. But perhaps they have access in other ways.
Panel: have you seen any evidence of access to psychiatry ?
AK: no. and no indication that it was important to them.
Panel: have you seen any evidence of access to psychiatry ?
AK: no. and no indication that it was important to them.
Panel: what do you think about MW's haste to prescribe given the delays in the NHS.
AK: I find it deeply troubling. I think it's badly advised and a rush to treatment.
Chair: [some discussion of logistics]. Now over to SJ, for re-examination.
AK: I find it deeply troubling. I think it's badly advised and a rush to treatment.
Chair: [some discussion of logistics]. Now over to SJ, for re-examination.
SJ: going back to fertility. Is there as a wider issue with fertility in those who identify as male?
AK: Yes, there is a wider issue here. Multiple pathways to consider and helping the child understand other options. How difficult or how easy.
AK: Yes, there is a wider issue here. Multiple pathways to consider and helping the child understand other options. How difficult or how easy.
AK: helping them explore different paths to being a biological parent. More considerations than 'do you want to give birth'.
SJ: returning to a question asked by the chair. About the timing of giving blockers.
SJ: returning to a question asked by the chair. About the timing of giving blockers.
SJ: In a response to a question asked by the Panel you replied 'misguided to start treatment and a haste to start could be detrimental and dangerous'. What rigour is required is by the clinician to get to a point where they recommend endocrine treatment should start?
AK: the decision really lies with the parent and the child. Our job as clinicians is that the decision has been thoughtfully and carefully explored. That they have fully explored what gender means to them and what gender roles are available. Its not our job to to conclude.
AK: that they should or shouldn't go on blockers. You need to establish a trusted relationship to discuss sensitive subjects. They have been given and understand all the information. We are never 'sure' we get to a point where we are confident
AK: that they are making the best decision they can at the time.
SJ: chair asked about child's understanding. Can you explain what steps the prescriber needs to take to establish and record that the child can take the decisions.
AK: a prescriber in our service
SJ: chair asked about child's understanding. Can you explain what steps the prescriber needs to take to establish and record that the child can take the decisions.
AK: a prescriber in our service
AK: would already have a great deal of information from the team and a full diagnostic report. Then they would confirm the information in asking questions to establish competence and understanding. They would have a strong base to start.
SJ: can you explain what you mean about diagnostic overshadowing?
AK: a child might describe gender dysphoria, but we don't know what else is going on in their lives, What other issues are going on. How are they doing at school, how it the family, what else is going on?
AK: a child might describe gender dysphoria, but we don't know what else is going on in their lives, What other issues are going on. How are they doing at school, how it the family, what else is going on?
AK: we need to understand what is happening with the child. There are those who argue that we don't really know about fully reversible. Reversible or not, there are side effects, a common one is lowering mood. The puberty blockers won't help with other mental health issues.
SJ: Back to the MDT. What do you think about that?
AK: I saw no sign of the normal functioning or working of a normal MDT.
SJ: now on the members of MW MDT. Reading out the recommended minimum credentials: (not repeated here, in the WPATH guidelines).
AK: I saw no sign of the normal functioning or working of a normal MDT.
SJ: now on the members of MW MDT. Reading out the recommended minimum credentials: (not repeated here, in the WPATH guidelines).
SJ: if not provided within the MDT, the MDT should ensure involvement or referral to the paediatric endocrinologist. Did you see any sign of involvement of paediatric endocrinologist ?
AK: No. GP of one patient involved Tavistock, but MW made no effort to engage with them
AK: No. GP of one patient involved Tavistock, but MW made no effort to engage with them
AK: or to involve paediatric endocrinologist .
SJ: have you seen any documentation setting out the background or qualifications of the MW MDT?
AK: no I have not.
SJ: point on time, in private care it may be quicker, it could be shortened but does that alter the assessment?
SJ: have you seen any documentation setting out the background or qualifications of the MW MDT?
AK: no I have not.
SJ: point on time, in private care it may be quicker, it could be shortened but does that alter the assessment?
AK: No, it does not alter the assessment, the communication, or the process.
SJ: no further questions.
Chair: back to the assessment stage at COI, in relation to time estimate, is 3 to 6 months, is that a minimum amount of time? What if you had limitless resources?
SJ: no further questions.
Chair: back to the assessment stage at COI, in relation to time estimate, is 3 to 6 months, is that a minimum amount of time? What if you had limitless resources?
AK: given limitless resources yes you could provide more information but it doesn't give you time to understand what the young people do with the information. What about social transition, changing name, uniform, pronouns. You would miss all of that information.
SJ: forgot one last question. How many patients are referred annually to Tavistock? What percentage of overall referral rate would those 1,2 or 3 children be.
AK: I couldn't say but it would be very small.
SJ: We will establish that through other sources.
AK: I couldn't say but it would be very small.
SJ: We will establish that through other sources.
Chair now discussing logistics for tomorrow.
The Panel will take the morning to consider medical evidence. They may take further evidence tomorrow from AK starting at 2:30 pm.
This is @justabaker17 Signing off for today.
@threadreaderapp unroll.
This is @justabaker17 Signing off for today.
@threadreaderapp unroll.
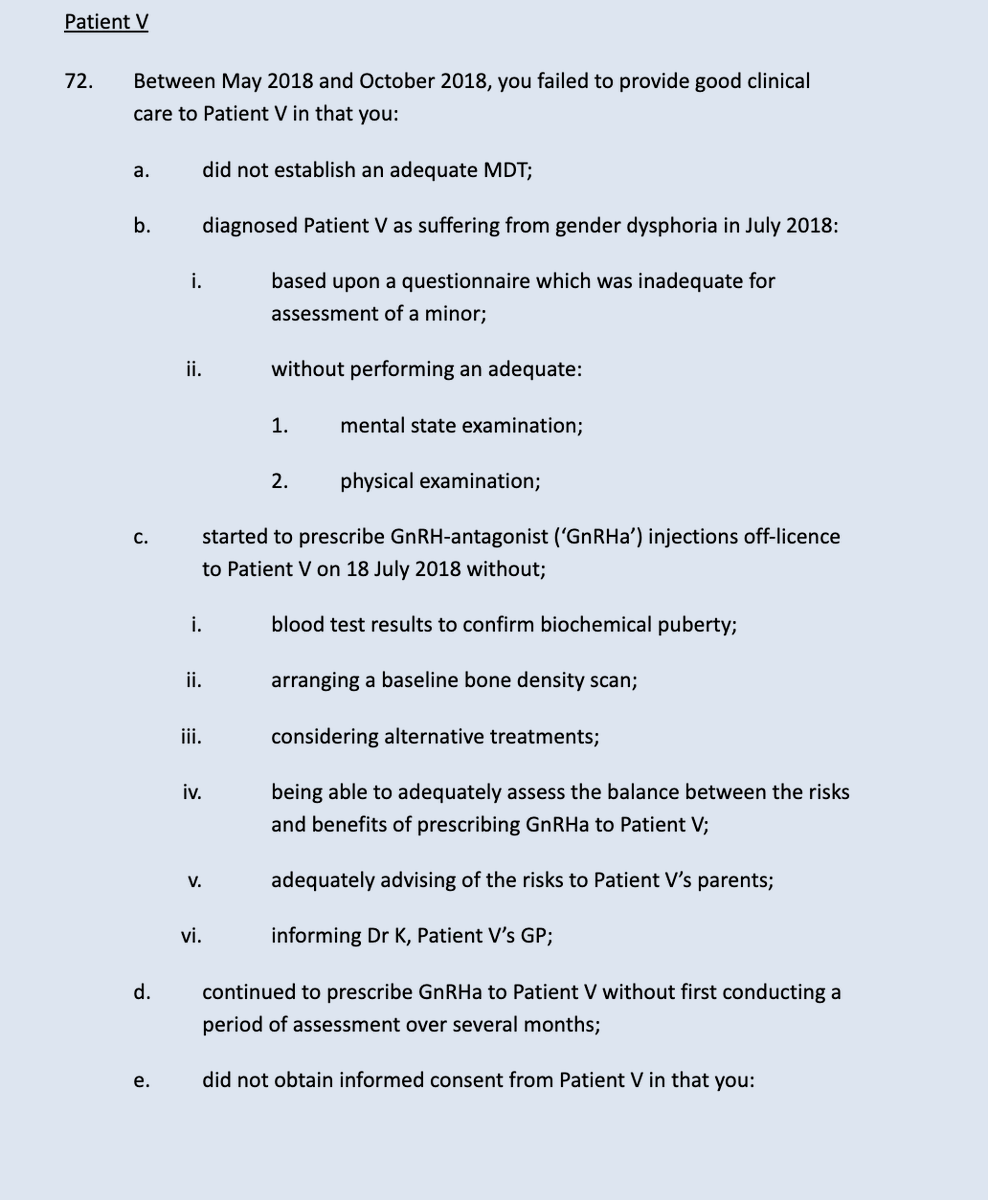
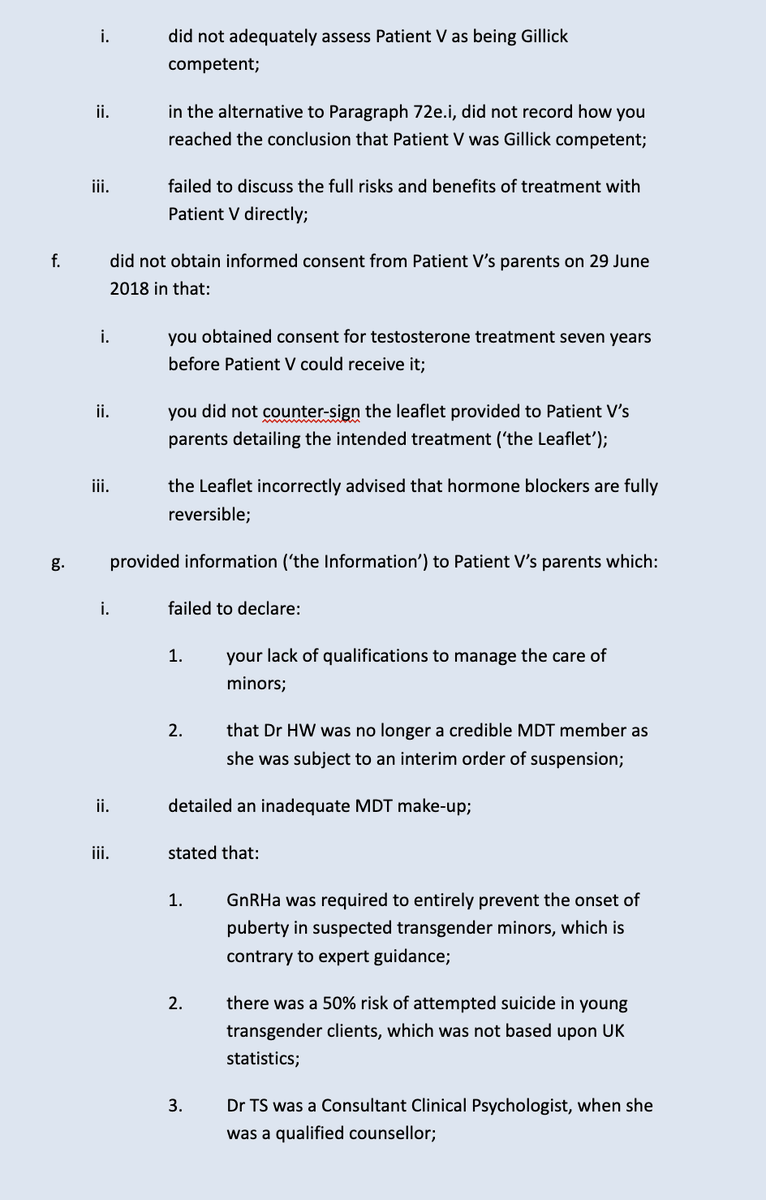
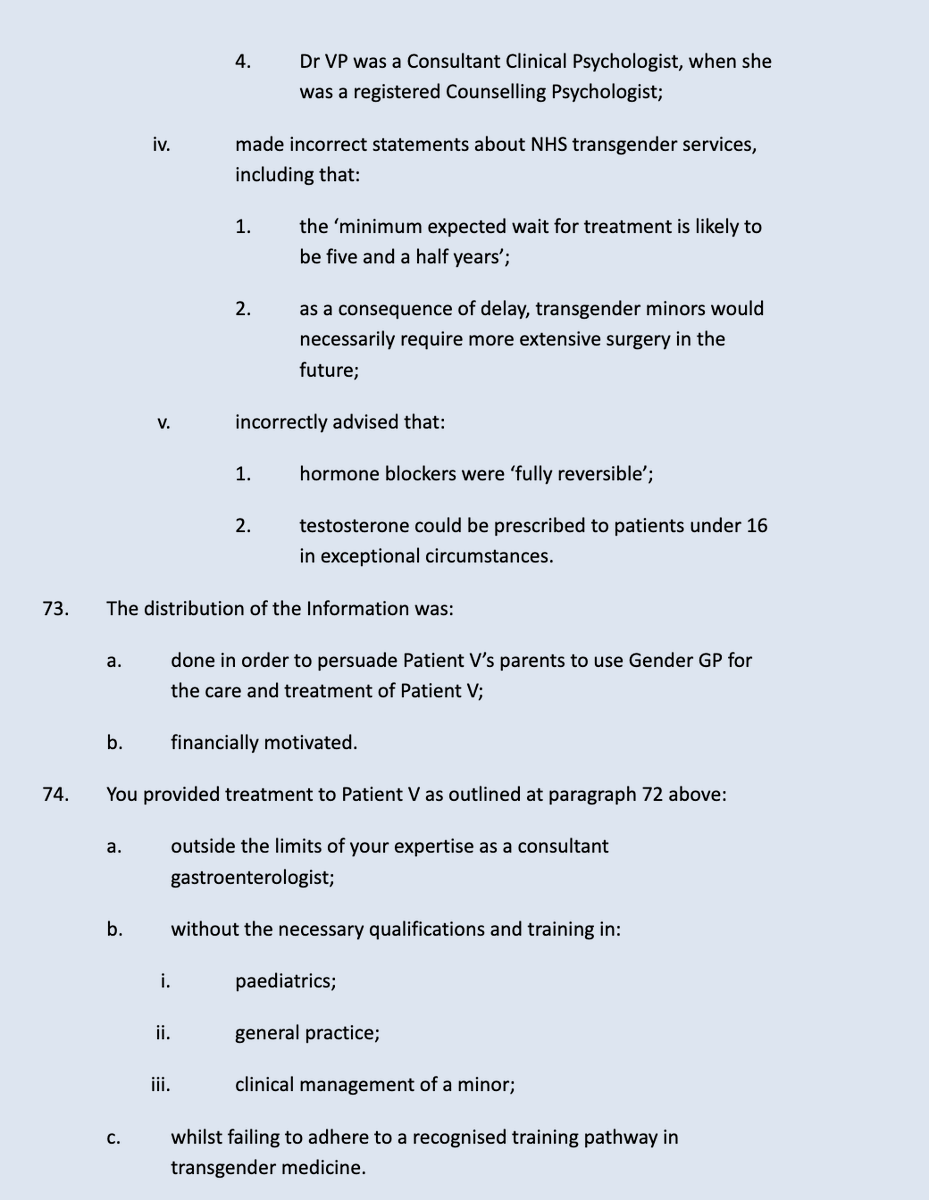
These are the allegations against Dr Michael Webberley in relation to Patient V: 
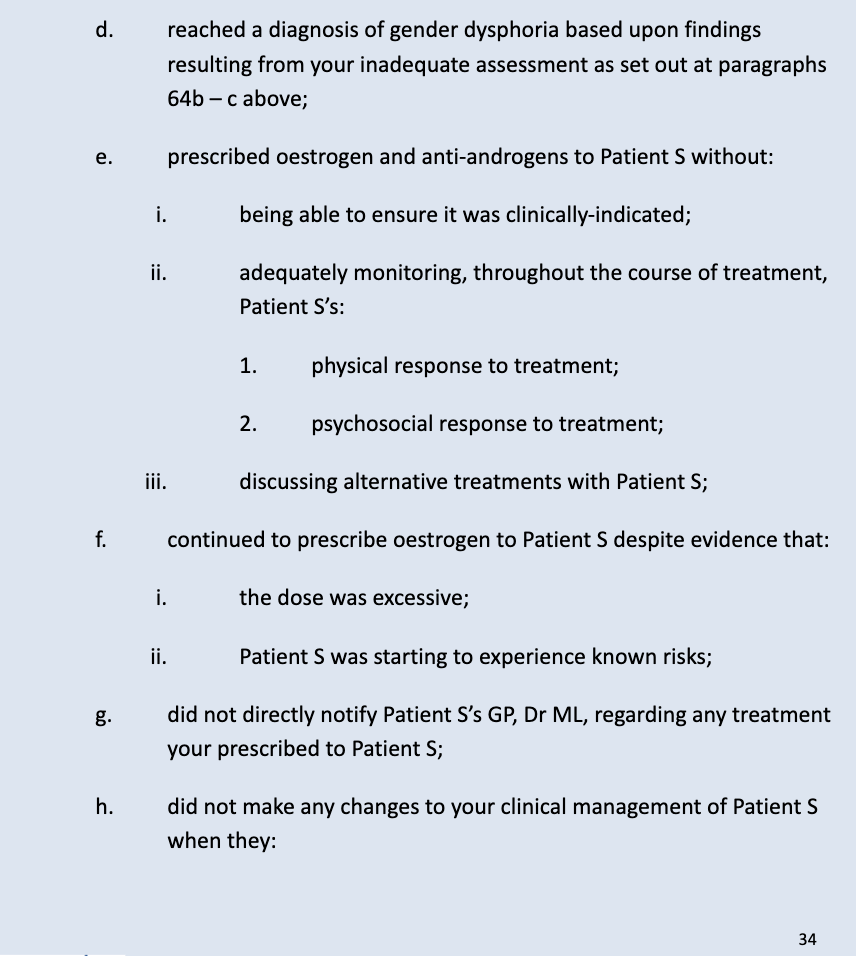
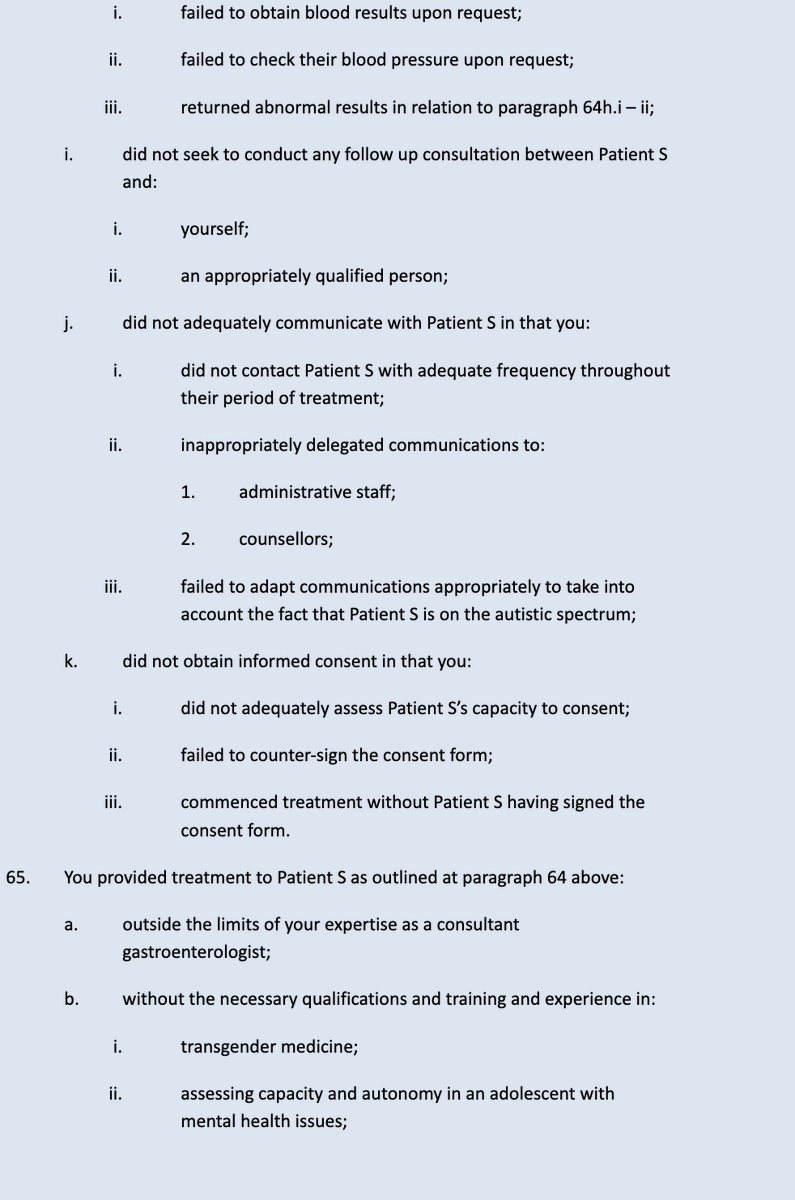
These are the allegations against Dr Michael Webberley in relation to Patient S:

• • •
Missing some Tweet in this thread? You can try to
force a refresh


