🚨Living with Covid #Access2Antivirals 🚨
Antiviral treatments are available to the 'Severely Immunosuppressed' a subset of the Clinically Vulnerable who remain at high-risk despite up to 5 vaccine doses.
🧵will cover how Vulnerable groups can access antiviral treatments.
1/
Antiviral treatments are available to the 'Severely Immunosuppressed' a subset of the Clinically Vulnerable who remain at high-risk despite up to 5 vaccine doses.
🧵will cover how Vulnerable groups can access antiviral treatments.
1/

Early antiviral treatment is a vital tool to prevent severe outcomes in high-risk people.
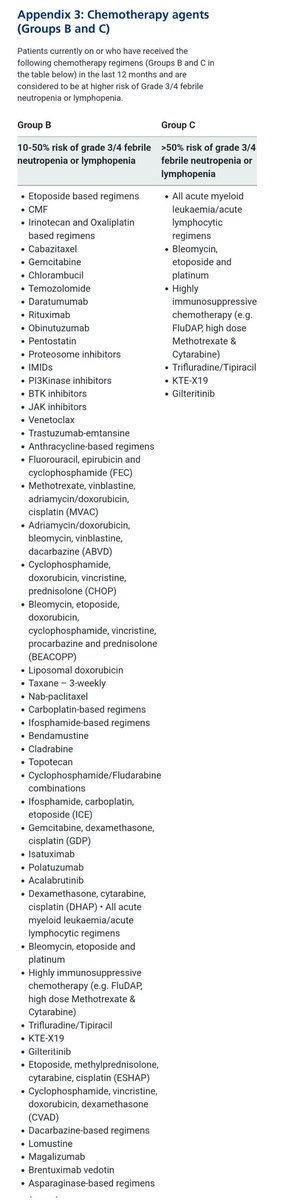
Currently only a small group who have poor immunity following vaccination are allowed to access them.
Please look through this list to see if you qualify:
england.nhs.uk/coronavirus/do…
2/
Currently only a small group who have poor immunity following vaccination are allowed to access them.
Please look through this list to see if you qualify:
england.nhs.uk/coronavirus/do…
2/

The 'Severely Immunosuppressed' group is smaller than those offered 5 vaccine doses & includes some never flagged as CEV.
So...
1) What should you do if you have Covid and DO qualify for antivirals?
2) What if you are Clinically Vulnerable/50+ and DON'T qualify on the list?
3/
So...
1) What should you do if you have Covid and DO qualify for antivirals?
2) What if you are Clinically Vulnerable/50+ and DON'T qualify on the list?
3/
What should you do if you have Covid and DO qualify for antivirals?
1. Make sure you have lateral flows at home. If you qualify for antivirals you can still order lateral flows for your own use.
gov.uk/order-coronavi…
4/
1. Make sure you have lateral flows at home. If you qualify for antivirals you can still order lateral flows for your own use.
gov.uk/order-coronavi…
4/

2. If you, or a member of your household, have Covid symptoms you* should test.
*Keep testing for a few days, especially if at all symptomatic. Try to Isolate / HEPA / ventilation & FFP3.
3. Even a pale positive on lateral flow is still a positive.
5/
*Keep testing for a few days, especially if at all symptomatic. Try to Isolate / HEPA / ventilation & FFP3.
3. Even a pale positive on lateral flow is still a positive.
https://twitter.com/cv_cev/status/1406638654353817601?t=FhHAJFBhZJnVjN--vORZdQ&s=19
5/
⏳️Your 5 day timer starts from your symptom start date⏳️
4. Report your result online.
(must be an NHS ordered test kit)
gov.uk/report-covid19…
In theory, this should be enough to trigger a referral.
Our experience shows you should also contact your GP or 111 / 119.
6/
4. Report your result online.
(must be an NHS ordered test kit)
gov.uk/report-covid19…
In theory, this should be enough to trigger a referral.
Our experience shows you should also contact your GP or 111 / 119.
6/

Ask to be referred you to your local Covid Medicines Delivery Unit (CMDU) for triage. (They should not refer you to each other.)
5. The CMDU should contact you within 48hrs.
If they do not, or you are on day 5, you need to follow it up.
Do not give up!
7/
5. The CMDU should contact you within 48hrs.
If they do not, or you are on day 5, you need to follow it up.
Do not give up!
7/

6. If during triage you are told that your symptoms are too 'mild' refer them to the guidance.
8/
england.nhs.uk/coronavirus/do…
8/
england.nhs.uk/coronavirus/do…
7. If you are told they only consider patients until day 6 or 7 refer them to this pathway.
By day 6/7 you would be limited to Remdesivir or 'off-label' (where a medicine used in a way different to that in the licence) access to the other treatments.
9/
england.nhs.uk/coronavirus/do…
By day 6/7 you would be limited to Remdesivir or 'off-label' (where a medicine used in a way different to that in the licence) access to the other treatments.
9/
england.nhs.uk/coronavirus/do…

⚠️ BEWARE of WEEKENDS ⚠️
Weekend access is generally poor. It appears to be a postcode lottery.
We are worried about the availability of services over the upcoming 4 day Bank Holiday weekend.
Some areas will offer treatment on day 6/7, but this is far from optimal.
10/
Weekend access is generally poor. It appears to be a postcode lottery.
We are worried about the availability of services over the upcoming 4 day Bank Holiday weekend.
Some areas will offer treatment on day 6/7, but this is far from optimal.
10/
8. If you are refused treatment and you do qualify you need to take it further try escalating within the hospital via your specialist team / PALS but be prepared to take it all the way to your local MP if all else fails by day 5.
nhs.uk/nhs-services/h…
11/
nhs.uk/nhs-services/h…
11/
We have heard that 10-15% of people who DO qualify can access these antiviral treatments.
Put another way, it means 85-90% can't access the antivirals.
We are highly concerned about this number!
12/
Put another way, it means 85-90% can't access the antivirals.
We are highly concerned about this number!
12/
What if you are Clinically Vulnerable/50+ and DON'T qualify on the list?
The only possibility is accessing treatments via the Panoramic trial.
Lots of people can qualify for the trial but only 450 participants are added daily, of which only 225 are given the treatments.
13/
The only possibility is accessing treatments via the Panoramic trial.
Lots of people can qualify for the trial but only 450 participants are added daily, of which only 225 are given the treatments.
13/

The demand has been high, due to the current surge.
However, this is currently closed for Easter...
It also appears to close over the weekends.
14/
However, this is currently closed for Easter...
It also appears to close over the weekends.
14/

The Panoramic trial has a screening process and either your GP, or a study nurse or doctor will assess your eligibility and ask for your consent.
If you do qualify you will have a 50:50 chance of being offered antivirals, which should arrive the next day.
15/
If you do qualify you will have a 50:50 chance of being offered antivirals, which should arrive the next day.
15/

Even if you don't receive the antivirals you will need answer questions online for 28 days and answer 3 phone calls to discuss with the trial team on days 7, 14 & 28.
16/
16/

We believe this constitutes health rationing.
Those 75+ should have been added to the antivirals list.
Plus, since treatments are already proven safe and effective for all Clinically Vulnerable / 50+, they should all have #Access2Antivirals through GPs and emergency GPs.
/END
Those 75+ should have been added to the antivirals list.
Plus, since treatments are already proven safe and effective for all Clinically Vulnerable / 50+, they should all have #Access2Antivirals through GPs and emergency GPs.
/END

@threadreaderapp unroll please!
• • •
Missing some Tweet in this thread? You can try to
force a refresh