
CPB 🧵pt4. Dessert course. Circ arrest.
Yes we know it’s a lifestyle.
But what IS it actually? Why do we do that to a person - stop blood flow to their whole body. Isn’t blood flow necessary? Or at least preferable?
#surged #meded #CTSurgery #CardioTwitter
Yes we know it’s a lifestyle.
But what IS it actually? Why do we do that to a person - stop blood flow to their whole body. Isn’t blood flow necessary? Or at least preferable?
#surged #meded #CTSurgery #CardioTwitter

To understand why we “circ arrest” someone- meaning arrest or stop the circulation to the whole body- we have to return to the basics of vascular surgery (bc cardiac surgery is kind of the ultimate #vascularsurgery 🙃)
it’s all about proximal and distal control
it’s all about proximal and distal control

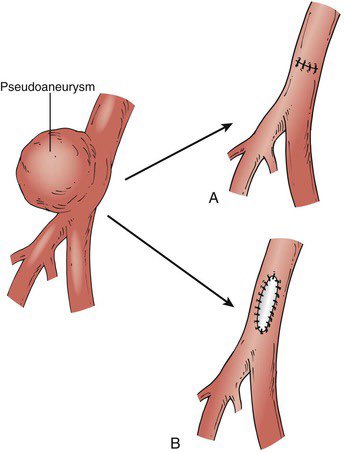
Let’s say you want to fix a psuedoanuerysm on the common femoral artery.
Well you need to get proximal and distal control with vascular clamps so that you can work on the area of interest.
Now while you’re working, the leg is a little sad 😔 but it’s got some collateral flow
Well you need to get proximal and distal control with vascular clamps so that you can work on the area of interest.
Now while you’re working, the leg is a little sad 😔 but it’s got some collateral flow
When we operate on the heart, it’s basically the same thing. Think about the circulation through the heart in series.
Proximal control: venous return side (drainage via venous cannula)
Distal control: blood exiting the heart (aortic cross clamp with flow beyond it)
Proximal control: venous return side (drainage via venous cannula)
Distal control: blood exiting the heart (aortic cross clamp with flow beyond it)

Of course when we exclude the heart and lungs with proximal and distal control, we need to offer a substitute- aka cardiopulmonary bypass which you’re already a pro at (see pts 1-3)

This principle of proximal and distal control applies everywhere, including the aortic arch.
Operating on blood vessels without control of the blood inside is not recommended, even for the most lionhearted.
Operating on blood vessels without control of the blood inside is not recommended, even for the most lionhearted.
So how is it that operating on the aortic arch can be HARDER than operating on the heart?
Well it took 3 🧵s but you know how to get proximal and distal control on the heart now.
What about for this aneurysm?
Well it took 3 🧵s but you know how to get proximal and distal control on the heart now.
What about for this aneurysm?

Sure just clamp before and after like this right?
Unfortunately:
1. What’s between the clamps is the 🧠 and patients like blood-> 🧠
2. What’s beyond the distal clamp is all the viscerals
3. It’s nearly impossible to clamp both those sites from any humane incision
Unfortunately:
1. What’s between the clamps is the 🧠 and patients like blood-> 🧠
2. What’s beyond the distal clamp is all the viscerals
3. It’s nearly impossible to clamp both those sites from any humane incision

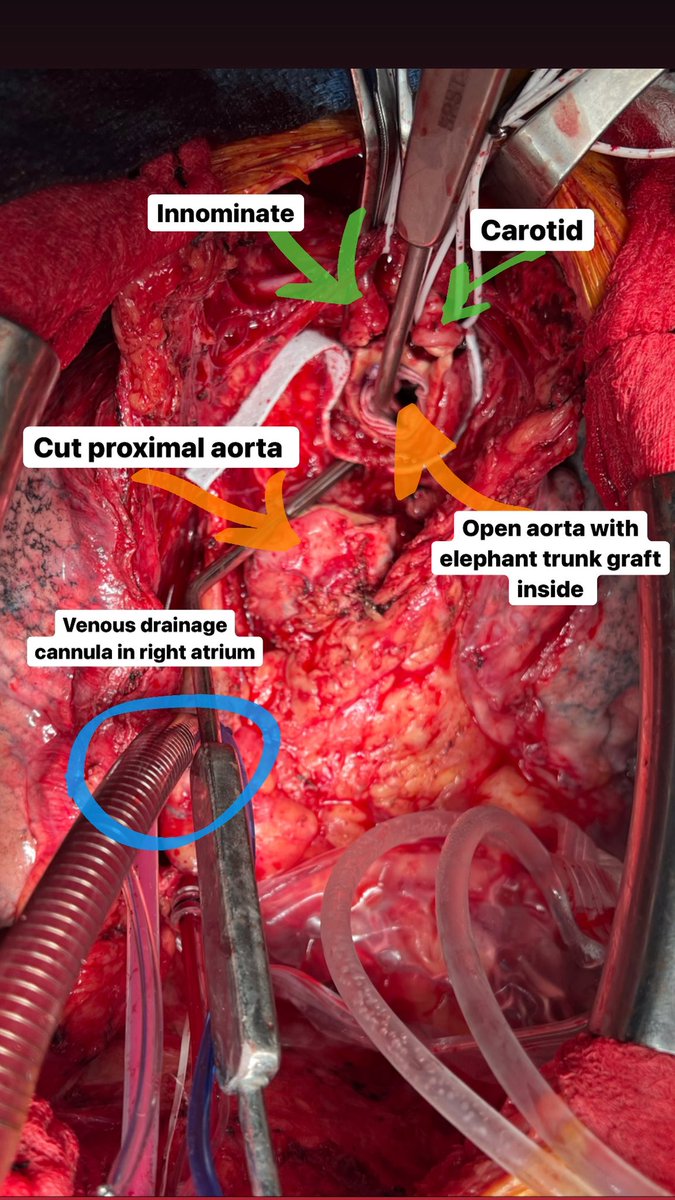
From a median sternotomy, we are able to access the arch (blue outline) to sew to.
Since we can’t safely clamp beyond the arch (and even if we could it doesn’t solve 🧠 perfusion), we need a way to sew to the distal anastomosis without being under water:
CIRC ARREST
Since we can’t safely clamp beyond the arch (and even if we could it doesn’t solve 🧠 perfusion), we need a way to sew to the distal anastomosis without being under water:
CIRC ARREST

When we open the aortic arch, we have to stop the heart and temporarily stop flow from the CPB circuit to the whole body.
Blood from the arch is drained via pump suckers and returned to the pump so we have a clear field to work.
Blood from the arch is drained via pump suckers and returned to the pump so we have a clear field to work.
Just like economics: it’s about supply and demand.
COOLing the patient down helps decrease metabolic demand during the time when no metabolic supply is being circulated.
Colder = less metabolic demand = longer safe circulatory arrest time
COOLing the patient down helps decrease metabolic demand during the time when no metabolic supply is being circulated.
Colder = less metabolic demand = longer safe circulatory arrest time

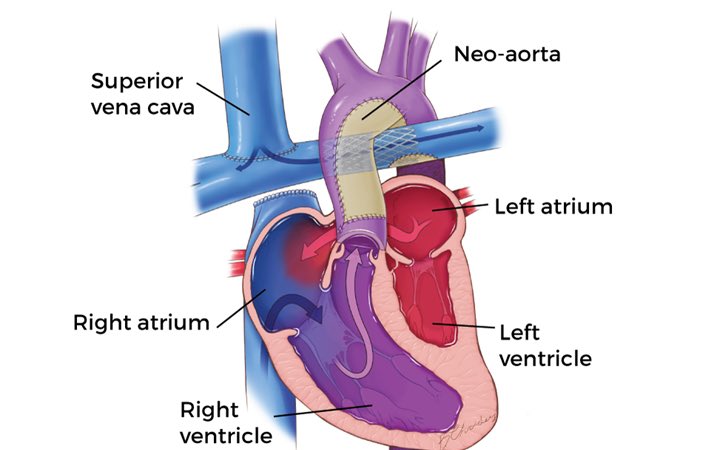
In congenital cardiac surgery on tiny babies needing aortic work, patients are routinely cooled to 15C which affords 30-40 minutes of safe arrest time- enough to do your aortic reconstruction in a Norwood operation -
often referred to as DHCA Deep Hypothermic Circulatory Arrest
often referred to as DHCA Deep Hypothermic Circulatory Arrest
In adults, we have a few more options since adult vessels are larger. For instance, we don’t HAVE to cannulate the aorta to flow - and turn everything off when we open the arch.
Instead, we can cannulate one of the head vessels and keep flow to the head:
Instead, we can cannulate one of the head vessels and keep flow to the head:

By clamping between the head and the arch and dropping the flow amount to just supply the head.
By keeping the head perfused, we don’t have to cool quite as low. Usually with “antegrade cerebral perfusion”, we can cool to 28C and shoot for the same arrest times for the body.
By keeping the head perfused, we don’t have to cool quite as low. Usually with “antegrade cerebral perfusion”, we can cool to 28C and shoot for the same arrest times for the body.

By cooling to 28, it’s MODERATE HCA.
Why not cool super low to protect the brain? Every maneuver has a cost - platelets and clotting factors go on strike at low temperatures.
Lethal triad in trauma: hypothermia, acidosis and coagulopathy.
Same in cardiac surgery!
Why not cool super low to protect the brain? Every maneuver has a cost - platelets and clotting factors go on strike at low temperatures.
Lethal triad in trauma: hypothermia, acidosis and coagulopathy.
Same in cardiac surgery!
Just to clarify something needlessly confusing: for cardioplegia we can flow antegrade or retrograde.
For regional cerebral perfusion, we can ALSO flow antegrade or retrograde! Nuances of these for another thread (or your CT fellowship apply here bit.ly/3JCSi8W)
For regional cerebral perfusion, we can ALSO flow antegrade or retrograde! Nuances of these for another thread (or your CT fellowship apply here bit.ly/3JCSi8W)
You don’t need to finish all your surgery on circ arrest time! Just enough to return to your homeostatic state of HAVING proximal and distal control.
Once the graft is sewn to the distal arch, it can be clamped and flow can resume to the head and body.
Once the graft is sewn to the distal arch, it can be clamped and flow can resume to the head and body.

Now you’re back to home base! Finish up any additional work during “rewarming” time and come off bypass once the patient is warm.
Happy circ arresting everyone!
Happy circ arresting everyone!

• • •
Missing some Tweet in this thread? You can try to
force a refresh




