
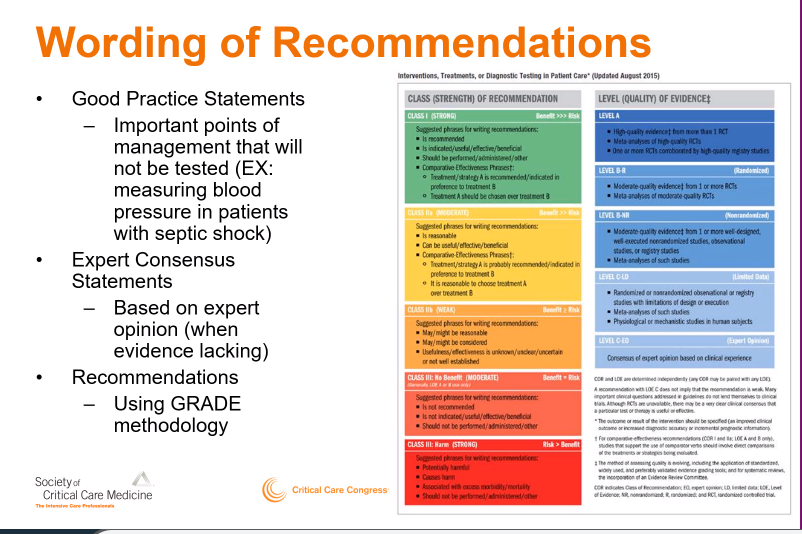
My next #PedsICU related #SCCM2022 topic is Pediatric TAXI-CAB Guidance. First @nellis discusses aims & general methods to create guidance for plasma & platelet transfusion.
Incredible expert team, but no nurses? Nurses administer🩸products and monitor for adverse events
1/
Incredible expert team, but no nurses? Nurses administer🩸products and monitor for adverse events
1/


• • •
Missing some Tweet in this thread? You can try to
force a refresh













