
🧵 1/n
Quantitatively review a national test and vaccine provider’s ongoing test positivity data.
Sources: Walgreen’s, 2020 US Census, Our World in Data
Yes, I’m embarrassed that @Walgreens has more comprehensive testing data than the @CDCgov, but that’s not my fault.
Quantitatively review a national test and vaccine provider’s ongoing test positivity data.
Sources: Walgreen’s, 2020 US Census, Our World in Data
Yes, I’m embarrassed that @Walgreens has more comprehensive testing data than the @CDCgov, but that’s not my fault.
All proportions are a 3d moving average.
Without any age considerations, is Walgreen’s testing over-sampling a particular cohort?
We start with age cohort vaccination rates from the CDC:
Without any age considerations, is Walgreen’s testing over-sampling a particular cohort?
We start with age cohort vaccination rates from the CDC:

For parsimony, I treat CDC 2 dose completed and Walgreen’s 2 dose or booster completed in the same category collapsing Walgreen’s 3 dose regimens into the 2 dose category.
1st Question: is Walgreen's data biased by "over-sampling" one group or the other (i.e., more vaccinated)?
1st Question: is Walgreen's data biased by "over-sampling" one group or the other (i.e., more vaccinated)?
Walgreen’s under-samples 1 dose individuals by quite a bit, but both vaccinated and unvaccinated are over-sampled with slightly more oversampling of unvaccinated.


Age Cohort Specific Check for Oversampling:
Walgreen’s data is more granular with a time component 🧐.
To compare to CDC numbers, we ignore the Walgreen’s time-based component.
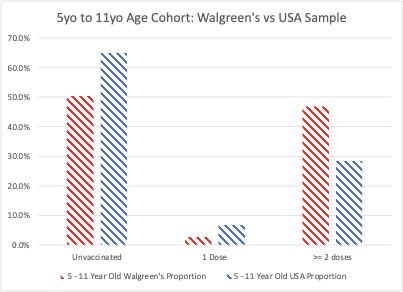
We can evaluate the Walgreen's sampling rate in each age cohort as compared to the US population
Walgreen’s data is more granular with a time component 🧐.
To compare to CDC numbers, we ignore the Walgreen’s time-based component.
We can evaluate the Walgreen's sampling rate in each age cohort as compared to the US population
For 5-11yo cohort, there is oversampling of the vaccinated cohort by a significant margin:

The oversampling of the vaccinated cohort still holds for the 12-17yo cohort (for some reason, Walgreens does not hold 1 dose information for that age cohort)


There is a significant change once we high 18-44yo cohort and beyond.
For the 18-44yo cohort, there is significant over-sampling of the unvaccinated and 1 dose recipients:
For the 18-44yo cohort, there is significant over-sampling of the unvaccinated and 1 dose recipients:


For the 45-64yo cohort, there is even more over-sampling of the unvaccinated:


For the 65yo+ group, the oversampling of the unvaccinated is substantial:


It's tempting to say that this is an artifact of an increasingly small proportion of unvaccinated in ascending age cohorts: so x number of tests has a bigger impact in biasing the ratio. Without having percentage of overall testing by cohort, the impact of this is hard to assess.
That said, we have enough to apply corrections to the posted positivity rates by age cohort, to see what the percent positivity is in each vaccination status after correcting for sampling bias.
Before we do that, let’s look at trends in each age cohort from 4/13 to 4/28. I pulled images on 4/13/22 and 4/28/22:

For reasons that are unclear, the positivity rate increases over the 2 week span in all age cohorts in all vaccination status categories.
Kids and Teens:
Kids and Teens:


Increased positivity rate over the 2 week span in all age cohorts in all vaccination status categories in adults:



Are these increases reflected in USA case rates in that interval?
4/13/2022: 118/M
4/28/2022: 171/M
Therefore, growth in Walgreen’s positivity rate outstripped USA case growth – could be marketing for all we know. I'm open to hypotheses.
4/13/2022: 118/M
4/28/2022: 171/M
Therefore, growth in Walgreen’s positivity rate outstripped USA case growth – could be marketing for all we know. I'm open to hypotheses.

The fun part: correct Walgreens positivity rates based upon their sampling bias.
To correct for sampling bias, just as we did to detect it, we collapse all categories for 2 doses or greater into one category of “2 or more doses”.
Reduces to "unvacccinated" vs "2 or more".
To correct for sampling bias, just as we did to detect it, we collapse all categories for 2 doses or greater into one category of “2 or more doses”.
Reduces to "unvacccinated" vs "2 or more".
1 dose was excluded as it is such a tiny proportion of the Walgreen’s sample (2.7%). USA rate for 1 dose is ~4x that.
The positivity rates by age and binary vaccination status WITHOUT any correction for sampling bias suggests higher positivity rate in all categories.
The positivity rates by age and binary vaccination status WITHOUT any correction for sampling bias suggests higher positivity rate in all categories.

After correcting for Walgreens sampling bias:
(Remember that these are “rates” so there is no base rate fallacy here. These are age cohort and vaccination status based.)
(Remember that these are “rates” so there is no base rate fallacy here. These are age cohort and vaccination status based.)

As a sanity check, is this consistent with what we see in other countries?
From the UK in February 2022 h/t @tlowdon and from the Icelandic MOH early Feb 2022 before they took their plots down (🧐):
From the UK in February 2022 h/t @tlowdon and from the Icelandic MOH early Feb 2022 before they took their plots down (🧐):


What is happening when we still have accounts and people claiming that vaccinated individuals are transmitting and getting infected less?
I covered early Omicron (BA1) transmission studies here:
I covered early Omicron (BA1) transmission studies here:
https://twitter.com/contrarian4data/status/1496620323201904648?s=20&t=Q1k_Wi-eeh9gUnSJW_1FFw
A follow up publication on Danish HH transmission looked at BA1 and BA2 specifically -- so same population and same methodology for a like-to-like comparison:
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
Effect of vaccination: this is a complicated table. Read the notes. In summary, referenced against transmission by “fully vaccinated”, booster vaccination reduction in transmission from BA1 moving into BA2 and is, on average, a 20% reduction.

Table: BA1 vs BA2 with BA1 being the “reference point”, being vaccinated ⬆️ your susceptibility to a BA2: noted by the authors.
Oddly, they didn't see ⬆️ onward transmission in vaccinated vs. BA1 -- paradoxical, BUT look at Denmark vs USA data curves and vaccine doses.
Oddly, they didn't see ⬆️ onward transmission in vaccinated vs. BA1 -- paradoxical, BUT look at Denmark vs USA data curves and vaccine doses.




Why are we seeing this?
The next few tweets are evidence-based, but speculative.
Imprinting: while not a new concern, people of stature are speaking publicly. Omicron specific mRNA boosters do not boost Omicron specific nAbs.
The next few tweets are evidence-based, but speculative.
Imprinting: while not a new concern, people of stature are speaking publicly. Omicron specific mRNA boosters do not boost Omicron specific nAbs.
https://twitter.com/contrarian4data/status/1515756838255353859?s=20&t=EXD97PE4qFIdIHM5_Wx67w
We now have strong evidence that vaccinated individuals do not develop anti-N antibodies to infection as frequently as when compared to unvaccinated individuals (40% vs 93%).
https://twitter.com/contrarian4data/status/1519151952201805826?s=20&t=EXD97PE4qFIdIHM5_Wx67w
At this point, it seems important for anyone who advocated for COVID vaccine mandates to walk it back ASAP.
Some are trying to walk it back by saying they were “saving hospital systems”.
Don’t dig your hole deeper.
Some are trying to walk it back by saying they were “saving hospital systems”.
Don’t dig your hole deeper.
That was never a reason to mandate this vaccine for populations that have never comprised a sizeable percentage of admissions.

Yes, boosting improved symptomatic disease, including severe disease, over Omicron in at risk populations. I saw it clinically.
Even if the duration and benefit of this was short-lived, it served a purpose.
Even if the duration and benefit of this was short-lived, it served a purpose.
Long term impact of potential imprinting? It's unclear, but risks are going to be greater in populations with more life-years left.
And to be clear, USA municipal data showing the aforementioned trends exists and people in power are looking -- you can't brush this under the rug.
And to be clear, USA municipal data showing the aforementioned trends exists and people in power are looking -- you can't brush this under the rug.
Pushing the vaccines as "pandemic enders" when they were never trialed to do so was a mistake.
People who are still perpetrating this fraud and sewing division are, at this point, ethically bankrupt
People who are still perpetrating this fraud and sewing division are, at this point, ethically bankrupt
https://twitter.com/DFisman/status/1518468658187620352?s=20&t=COrxfpBhkG0VBau56auq9A
As some have asked, since we’re looking at positivity rates, once we ascertain that there’s no sampling bias pushing Walgreens to markedly overestimate vaccinated disease burden, we don’t absolutely need to correct for any “sampling bias”. Indeed, it overstates effect.
See here:
See here:
https://twitter.com/contrarian4data/status/1522632601973846017
• • •
Missing some Tweet in this thread? You can try to
force a refresh









