
Dad bleed to death 5 years ago today.
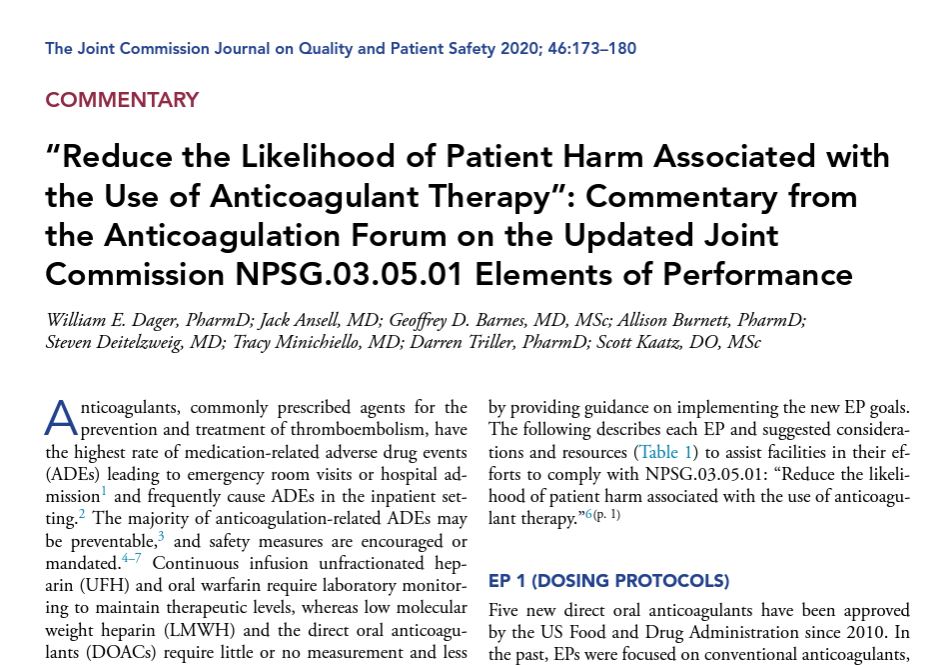
I usually prefer to remember his life, but ever since I got the letter from @CVSHealth PBM Caremark saying I couldn't continue on the anticoagulant with the lowest risk of major bleeding, Dad's final moments have been heavy on my mind. 🧵
I usually prefer to remember his life, but ever since I got the letter from @CVSHealth PBM Caremark saying I couldn't continue on the anticoagulant with the lowest risk of major bleeding, Dad's final moments have been heavy on my mind. 🧵

I got the call around 4am from my parent’s neighbor saying there was blood everywhere in Dad’s bedroom. Mom was hysterical. EMS were on the scene. 2/
Dad was stabilized at their small rural hospital before being transported an hour to a large academic hospital. He had a major bleed in his lungs. Despite best efforts over the next 48 hours, he had one final traumatic bleed out which could not be stopped.3/
I wish it had been a peaceful death. It was not. Dad essentially drown in his own blood. Thank goodness I was with him in ICU instead of Mom when he suddenly began to aspirate a mass volume of blood. Bless the healthcare professionals who deal with this kind of trauma everyday.4/
Bleeding can occur even with optimal anticoagulation management. I do not blame the drug. I will never name the brand for that reason. But because bleeding is a known risk of ALL anticoagulants, that’s why I only want my doctor—not my insurance PBM—to manage my medication. 5/
Imagine then how I felt when I got the letter from @CVSHealth knowing that the anticoagulant they were FORCING me to switch to was NOT the one with the lowest clinical bleed risk!
They knew better than my own hematologist of 18 years which anticoagulant was best for me?! 6/
They knew better than my own hematologist of 18 years which anticoagulant was best for me?! 6/

The clinical evidence is VERY clear. 2 hematologists in my own care both agreed this was the drug I needed to both prevent recurrent clot & lower my risk of major bleeding. Knowing this how could I feel good about CVS Caremark forcing me to change anticoagulants? 7/



This forced change filled me with great anxiety. I requested to stay on my medication as I'd been successful & stable on it for 8 years. But the stated approval criteria required I first take & FAIL the new drug.
Failure on an anticoagulant = clot or bleed.
8/
Failure on an anticoagulant = clot or bleed.
8/

And notice after 'failing' the new medication with an adverse event & only then being allowed to go back & continue on the drug which I'd been successful & stable on the past 8 years, it would be approved at a higher tier! For me, that's an extra $2,400 annually. Some choice. 9/
I had already picked up the new medication from the drug store & ready to change, when because of 2 thromboembolic events among patients who had switched, my NC plan overrode Caremark & reinstated Eliquis to their formulary. I cried. To depend on a pill makes one vulnerable.10/

Anticoagulants are the #1 drug class for adverse events. They cause more ER visits than even opioids & are serious--48% result in a hospital admission.
Yet PBM Caremark willy-nilly casually switched at-risk patients anticoagulants for non-medical reasons.
Egregious abuse. 11/
Yet PBM Caremark willy-nilly casually switched at-risk patients anticoagulants for non-medical reasons.
Egregious abuse. 11/

Numerous federal efforts prioritize reducing anticoagulant harm.
"anticoagulation requires a careful balance between thrombotic & hemorrhagic risks & is easily influenced by a multitude of factors" @HHSGov
Yet a PBM can take anticoagulation so lightly? Remarkable hubris. 12/
"anticoagulation requires a careful balance between thrombotic & hemorrhagic risks & is easily influenced by a multitude of factors" @HHSGov
Yet a PBM can take anticoagulation so lightly? Remarkable hubris. 12/

The Joint Commission @TJCommission has made reducing anticoagulant harm a top National Patient Safety Priority.
"The majority of anticoagulation ADAs may be preventable"
Yet PBM CVS Caremark proceeded with an action which 16 nonprofits warned would increase risk of harms? 13/
"The majority of anticoagulation ADAs may be preventable"
Yet PBM CVS Caremark proceeded with an action which 16 nonprofits warned would increase risk of harms? 13/
When a multi-billion dollar corporation controlling 1 in 3 Americans drug access thumbs their nose at American Society of Hematology & American College of Cardiology experts telling them in person & in writing they risk patient safety, a federal investigation is needed why. 14/


And to think, CVS Caremark was willing to risk patient harms simply because they got a slightly higher rebate from one drug manufacture than another! Eliquis & Xarelto retail for about the same price. The ONLY possible reason to prefer one on formulary is profit kickback. 15/


And harms did happen--thromboembolic stroke & clinically significant bleeds. I'm aware of 8 events in 5 states, one in a 26 year old patient!!! These were stable patients forced to switch anticoagulants for non-medical profit motivated reasons! 16/ fox13memphis.com/news/local/doc…
Because this is now hitting the news, rumor is Eliquis will be added back to formulary July 1. Good for patients going forward. It shouldn't have taken negative PR to make it happen. When docs told Caremark in DECEMBER 'patients need this drug' that should have been enough. 17/
Reminder these organizations told PBM Caremark they they were 'gravely concerned' & CVS was making a 'dangerously disruptive' decision risking patient safety. @CVSHealth not only ignored them flat out but even promoted the PBM executive who met with some of them. Astonishing.18/

The rub: As a patient whose employer plan contracts w/ Caremark as PBM, I am a captive PBM consumer & my family will need to continue to rely upon this company. I fear there may be a price to pay for my advocacy based on what's happened so far. 19/ managedhealthcareexecutive.com/view/how-a-for…
Anticoagulants should be a protected drug class w/ all FDA approved drugs on formulary.
Prohibit non-medical switching.
It is astounding that a corporation can essentially practice medicine by coming between the evidence-based care decisions made between doctor & patient. 20/
Prohibit non-medical switching.
It is astounding that a corporation can essentially practice medicine by coming between the evidence-based care decisions made between doctor & patient. 20/
Federal investigation into this serious patient safety matter is required without delay. Without strong protections patients will continue to be at risk. 21/ @linakhanFTC @FTCPhillips @RKSlaughterFTC @CSWilsonFTC @alvarombedoya @SenFinance @SenBlumenthal @RonWyden @SenatorBurr
Thank you for reading this thread on this day I remember my Dad. All patients deserve to have the decisions made between them & their doctor respected. 22/
#MedTwitter #CardioTwitter #Cardiology #StopTheSwitch #NoBigDeal #TwitterRx
onlinelibrary.wiley.com/doi/full/10.10…
#MedTwitter #CardioTwitter #Cardiology #StopTheSwitch #NoBigDeal #TwitterRx
onlinelibrary.wiley.com/doi/full/10.10…
• • •
Missing some Tweet in this thread? You can try to
force a refresh











