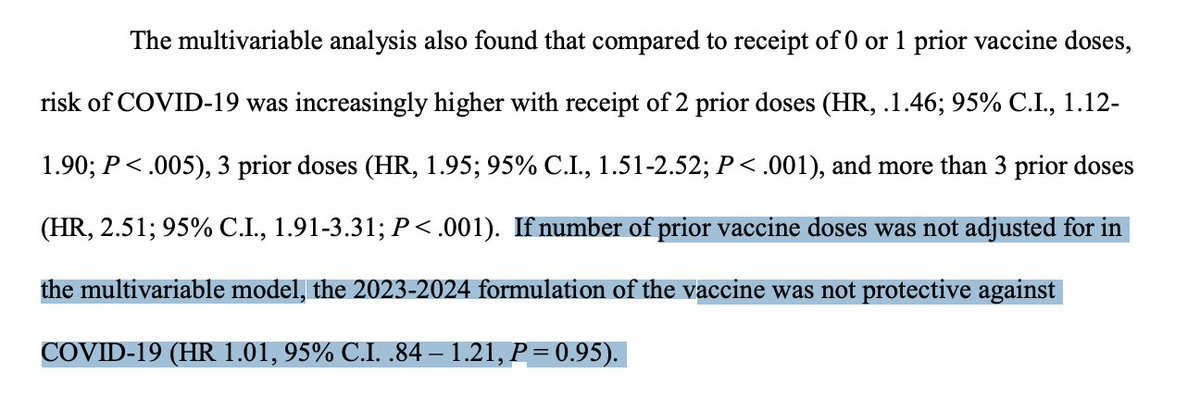
This new JAMA study is worth discussing. It found that, this winter, vax effectiveness in 12-15 yos dropped to 0% after 3-5 months & vaccinated were MORE likely to test+ at month 7. May be confounded (see🧵)
But I don't see this as good reason for boosters
jamanetwork.com/journals/jama/…
But I don't see this as good reason for boosters
jamanetwork.com/journals/jama/…
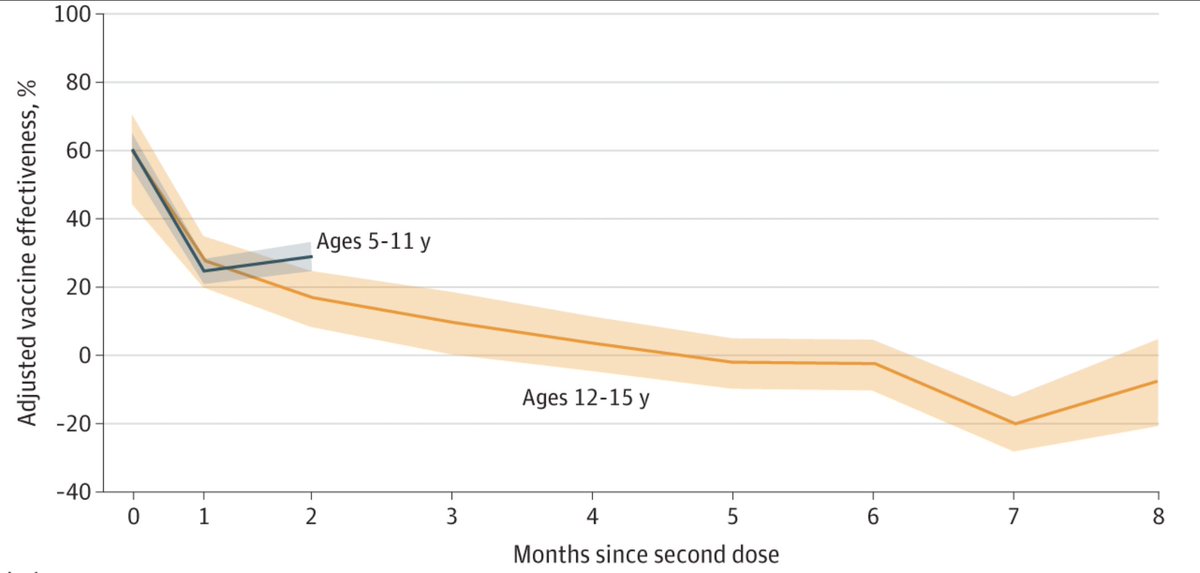
I think the most likely confounder here which could lead to the calculated negative effectiveness is higher amount of immunity from prior infection in the unvaccinated group. It could also be related to different behaviors in the two groups. Need randomization to sort this out
Remember, we have seen the same pattern of negative effectiveness in 5-11 year olds in NY so I don't think what we are seeing in the JAMA study is limited to 12-17 year olds
Also, remember, this is only looking at infection rate and not severe disease rate
Also, remember, this is only looking at infection rate and not severe disease rate

Some have suggested negative effectiveness may be due to imprinting leading to an increased risk of infection among vaccinated over time, but until randomized data or other more convincing data are available I'm not ready to latch onto that theory, though it's hard to rule out
Almost all kids are very low risk from this disease & especially since protection against infection wanes quickly, we need risk benefit analyses of protection against severe disease vs vaccine adverse events for each dose, esp since >3/4 of kids have immunity from prior infection
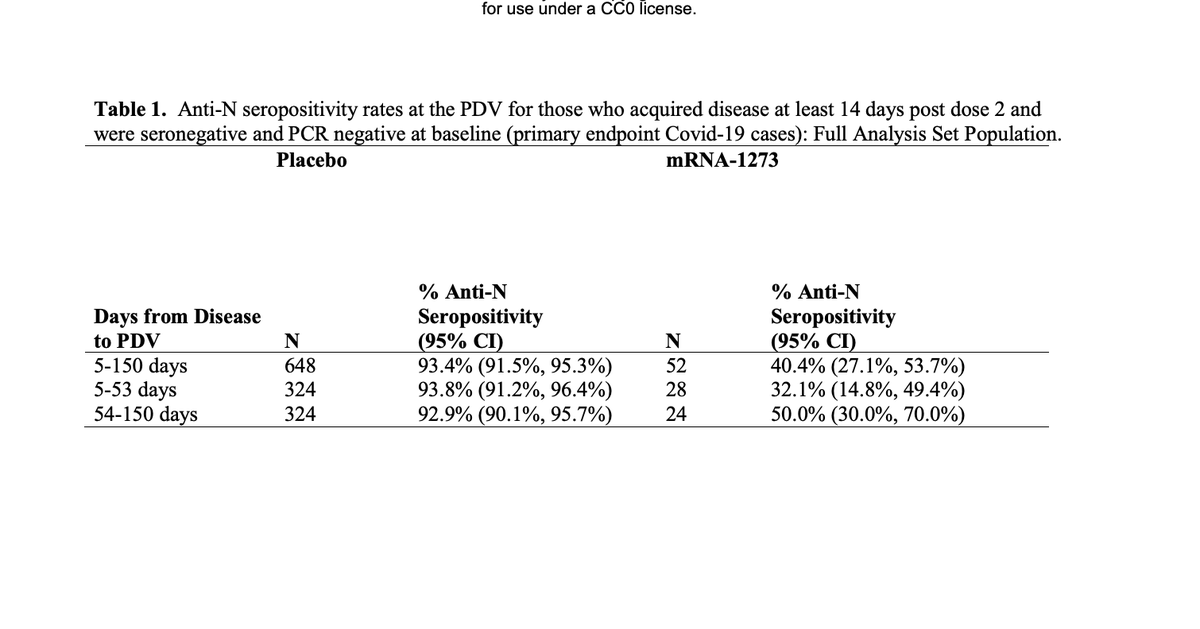
Re imprinting: some data we have so far to support this are randomized moderna data showing vaccinated less likely than unvax to develop anti-nucleocapsid antibodies after infection (40-50 vs >90%) but I don't think we know what this means clinically yet
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
• • •
Missing some Tweet in this thread? You can try to
force a refresh