1/ NOT THE THREAD DIGITAL HEALTH WANTS TO READ, BUT THE THREAD IT NEEDS TO READ. Walk with me…🧵
2/ Many people know about the darling of digital health — Livongo. Arguably the highest profile digital health company ever due to an $18.5 billion dollar merger with Teladoc back in 2020. medcitynews.com/2020/10/telado…
3/ Livongo is/was known for its digital diabetes program. Unfortunately, the market never demanded that Livongo prove their program works. By the time Teladoc published an RCT, it turned out that the program was NO BETTER THAN USUAL CARE. ncbi.nlm.nih.gov/pmc/articles/P…
4/ Maybe that’s why Teladoc is dropping in value? 🤷🏼♂️ healthcaredive.com/news/teladoc-r…
5/ Or what about Omada? They are another digital chronic disease unicorn. Did you know they recently published the largest digital diabetes prevention study…of all time! Honestly, kudos to them for doing it. globenewswire.com/news-release/2…
6/ Here is the registered study protocol for PREDICTS clinicaltrials.gov/ct2/show/NCT03…
7/ Study was a 12-month randomized control trial of a digital diabetes prevention program.
D-DPP: 52 weekly sessions, lifestyle coaching, virtual peer support, and behavior tracking tools. N=299
Control: single-session small-group diabetes-prevention education class; N=300
D-DPP: 52 weekly sessions, lifestyle coaching, virtual peer support, and behavior tracking tools. N=299
Control: single-session small-group diabetes-prevention education class; N=300
8/ Despite the high level of support in the d-DPP arm, the participants only achieved a trivial improvement in glycemia (-0.08% A1c compared to control) and modest improvement in weight (-5.5% d-DPP vs -2.1% congrol) at 12 months.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…

9/ So why all the fuss? Because being no better than usual care is not a scientific achievement or progress, and I’ll let you decide if that is worth $18 billion. Also, stop digitizing the diabetes prevention program!!! It’s over 20 years old!! The science has progressed!
10/
FOR EXAMPLE ⤵️
Pharmacy-led ketogenic diets have far better data for glycemic control. nature.com/articles/s4146…
Virta has demonstrated a more effective digital diabetes/predm program. frontiersin.org/articles/10.33…
FOR EXAMPLE ⤵️
Pharmacy-led ketogenic diets have far better data for glycemic control. nature.com/articles/s4146…
Virta has demonstrated a more effective digital diabetes/predm program. frontiersin.org/articles/10.33…
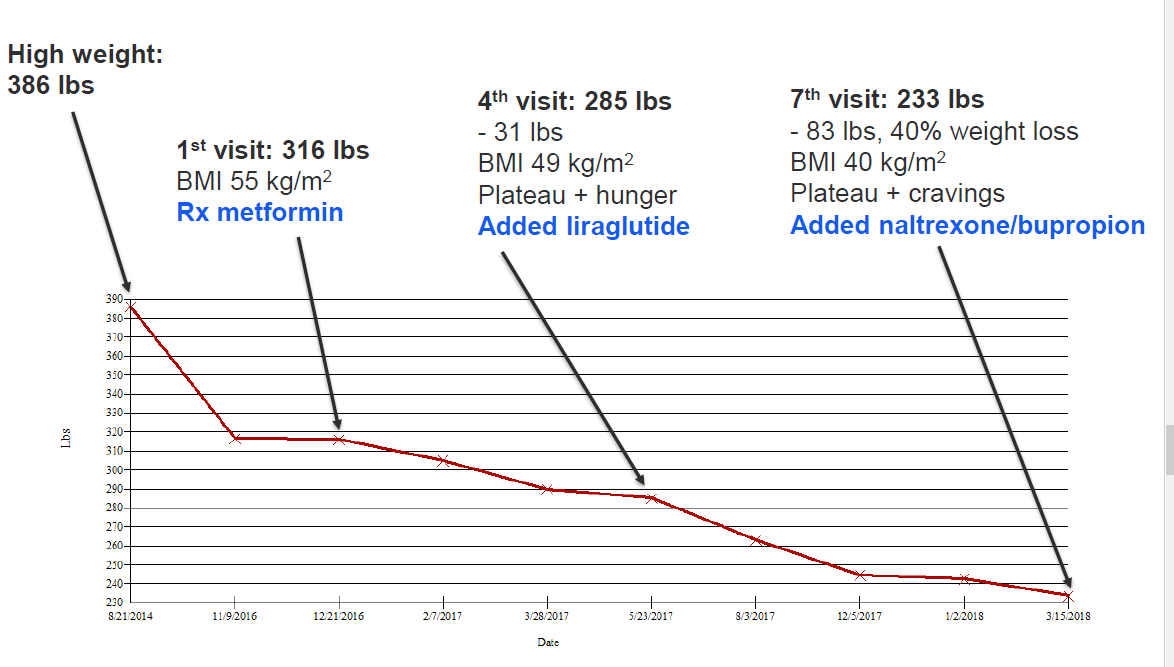
11/ Heck, I could put people on a single drug, close my eyes, and outperform all the programs above. #tirzepatide diabetes.org/newsroom/press…
12/ While I appreciate the efforts to finally start validating some digital health programs that have been around for a while, the validation should have happened sooner. Also, the results should be more impressive to warrant their current valuations (IMO).
13/ The point is that we should not lower the scientific standard for digital health companies. It’s time for digital health to put its money where its mouth is. Because lives are at stake, and no one gets a pass. [end]
• • •
Missing some Tweet in this thread? You can try to
force a refresh