Big #LongCovid paper out with a lot of new insights (n=78k)!
-76% of LC patients were not hospitalized (!!)
-82% of female patients non-hospitalized vs 68% males
-36-50 year olds were the highest risk age group
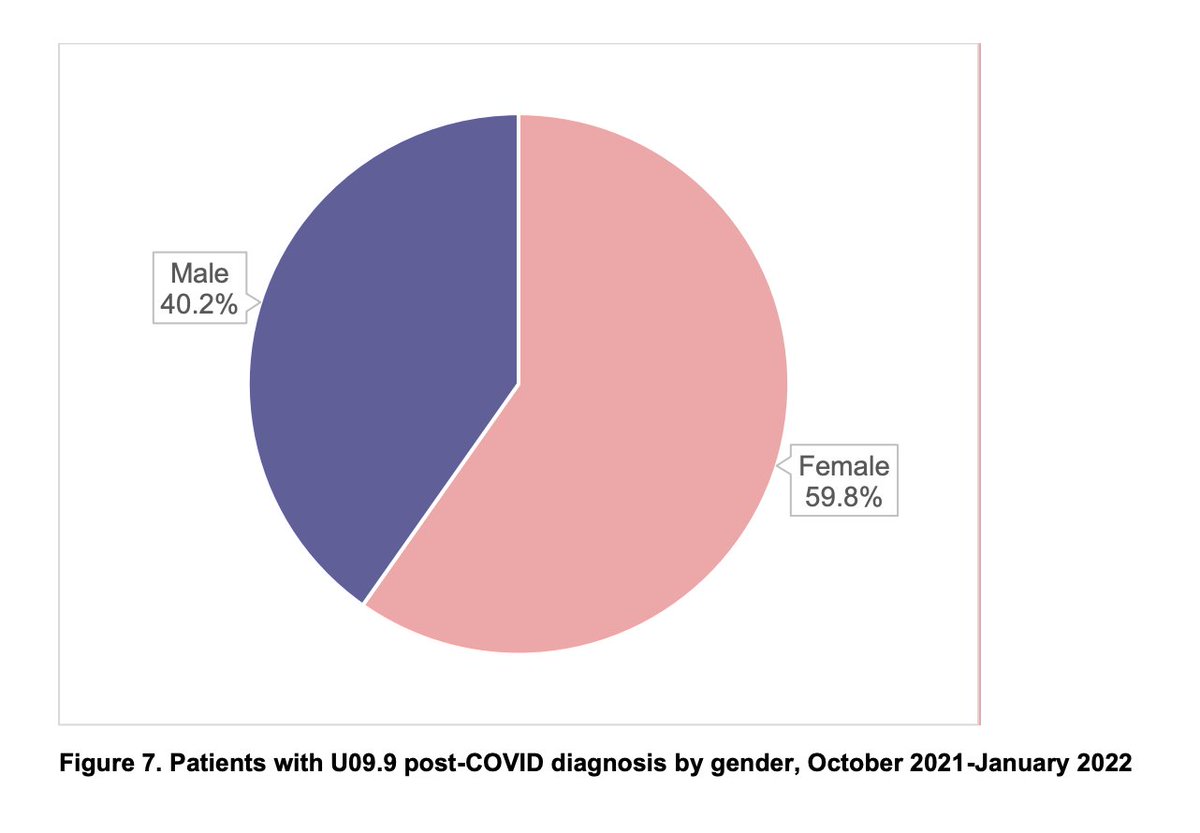
-59.8% of patients female; 46.2% male
s3.amazonaws.com/media2.fairhea…
1/
-76% of LC patients were not hospitalized (!!)
-82% of female patients non-hospitalized vs 68% males
-36-50 year olds were the highest risk age group
-59.8% of patients female; 46.2% male
s3.amazonaws.com/media2.fairhea…
1/
-31% had no pre-existing condition
-Heartbeat irregularities were more common in age 13-22 (possibly dysautonomia)
-Myopathies (diseases that affect the muscles that control voluntary movement) were 11.1x more common in #LongCovid compared to the same population pre-COVID!
2/
-Heartbeat irregularities were more common in age 13-22 (possibly dysautonomia)
-Myopathies (diseases that affect the muscles that control voluntary movement) were 11.1x more common in #LongCovid compared to the same population pre-COVID!
2/
On average, patients with #LongCovid had higher
HHS-HCC risk scores after COVID-19 than before.
HHS-HCC risk scores identify which patients are likely to consume more healthcare resources & incur more healthcare-related costs in the long run.
3/
HHS-HCC risk scores after COVID-19 than before.
HHS-HCC risk scores identify which patients are likely to consume more healthcare resources & incur more healthcare-related costs in the long run.
3/

As other studies have found, there is a gender difference, but it heavily depends on age group! For children under 12 and adults over 50, the chance of getting #LongCovid is almost equal between male and female patients.
5/
5/

Obstructive sleep apnea was the most common sleeping diagnosis, which seems weird to me. Wonder if any of these are actually central apnea?
6/
6/

A few diagnoses were highlighted as uncommon but potentially serious, with a large difference between pre- & post-COVID.
These included myopathies (11.1x more common), diseases affecting the interstitium (4.8x more), pulmonary embolism (2.6x), other brain disorders (2x).
7/
These included myopathies (11.1x more common), diseases affecting the interstitium (4.8x more), pulmonary embolism (2.6x), other brain disorders (2x).
7/

Breakdown of "other disorders of the brain", which seems to be ME/CFS-type manifestations, metabolic encephalopathy, and encephalopathy.
8/
8/

• • •
Missing some Tweet in this thread? You can try to
force a refresh