Have to say, I'm quite astonished having watched the recent CDC presentations on fulminant hepatitis in children. So much discussed on Adv, with a passing mention of COVID serology (not yet done). Not a single biopsy with Adv in the liver- yet children treated with antivirals.🧵
I'm a trained clinician and epidemiologist. During my clinical training, I'd have had to rigorously justify why I did any test (to avoid incidental positives), why I made a specific diagnosis on a patient, and why I treated for it. I can't really fathom what's happening here.
1) How plausible is it that Adv is doing this?
Let's look at Adv here- Adv 41F has *never* caused this. Other Advs have *never* caused hepatitis in healthy children.
2) Did we at least find Adv in the liver in these cases?No. This is the key feature of Adv fulminant hepatitis
Let's look at Adv here- Adv 41F has *never* caused this. Other Advs have *never* caused hepatitis in healthy children.
2) Did we at least find Adv in the liver in these cases?No. This is the key feature of Adv fulminant hepatitis
If there's no evidence of Adv in the actually tissue affected- the literal *diagnostic criterion* for fulminant hepatitis- you simply cannot diagnose it.
The biopsies suggest some sort of auto-inflammatory process rather than direct infection.
The biopsies suggest some sort of auto-inflammatory process rather than direct infection.
On the other hand, this could be post-COVID. Why haven't we specifically evaluated this? Given we actually know SARS-CoV-2 causes hepatitis- both with direct infection, and post-infection (as part of MIS-C but also without). Many reports already show this.
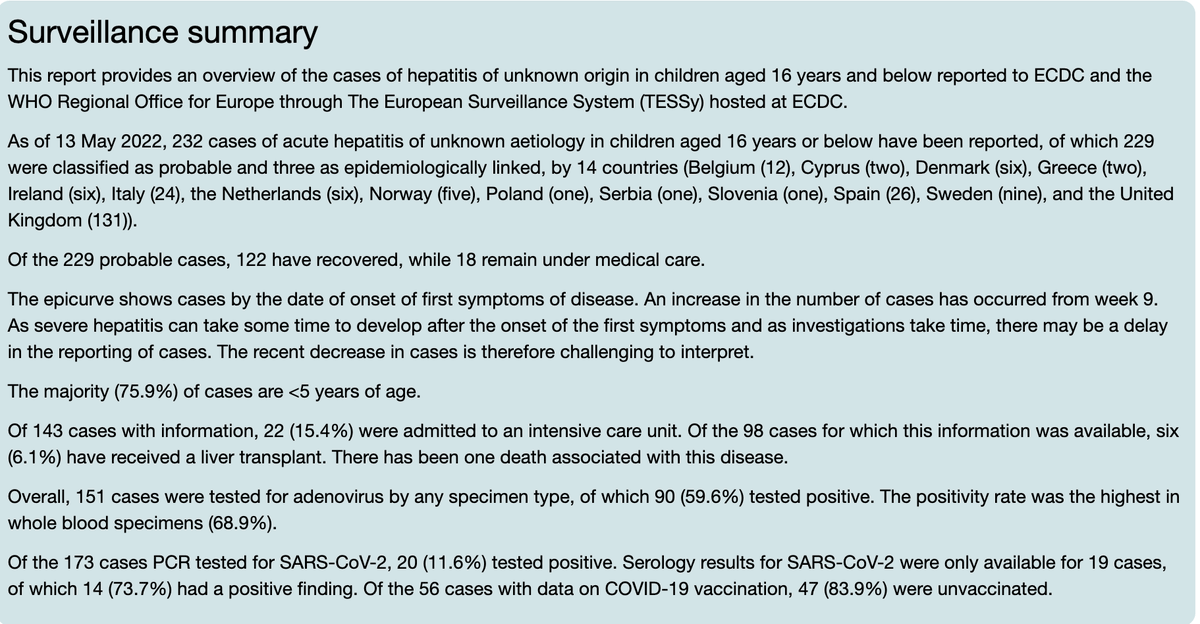
The positivity for SARS-CoV-2 is in line with previous reports for MIS-C. And seropositivity in the very limited sampling we've seen is considerably high. And Israel and Austria have both reported past/recent SARS-CoV-2 infection in all cases.
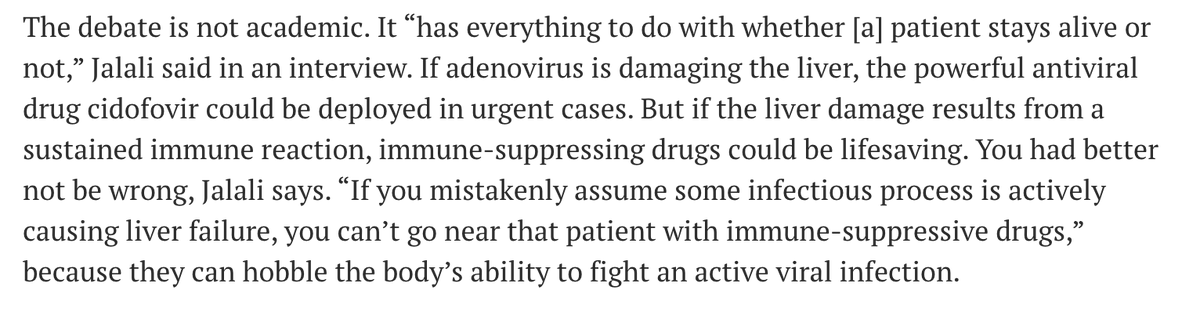
Yet, we've gone down looking for a pathogen that's never done this before, & doesn't even fulfil the diagnostic criteria. And patients are being treated for this nevertheless? The treatment for several patients was cidofovir (an antiviral)
What worries me even more is that this is a continuing education teaching session on paediatric hepatitis from the CDC. Shouldn't we be teaching more critical thinking in clinical training? Any clinician would be hard pressed to justify the thinking and decisions made here.
Why are clinicians making this diagnosis, without the actual diagnostic criterion needed for this consulting with others who've treated this as post-inflammatory/post-COVID? Austria, Israel & Italy have done this- treated with immunomodulation.
Isn't it worth understanding their experience? Both Austria and Israel had previous COVID-19 in all cases. Isn't it worth understanding the clinical course, what the thinking behind the diagnosis was, and whether it improved with steroids?
It seems bizarre to me that we have this clinical entity that some countries are treating as post-infectious inflammatory, while others are treating with antivirals despite no evidence that the viral agent is causal. And without evaluating one of the more likely causes.
Had I presented this on grand rounds I'd have been hard pressed to justify:
1. Why I considered Adv as my 1st differential given lack of previous evidence & more plausible causes
2. How I diagnosed and treated for Adv fulminant hepatitis without the diagnostic criterion being met
1. Why I considered Adv as my 1st differential given lack of previous evidence & more plausible causes
2. How I diagnosed and treated for Adv fulminant hepatitis without the diagnostic criterion being met
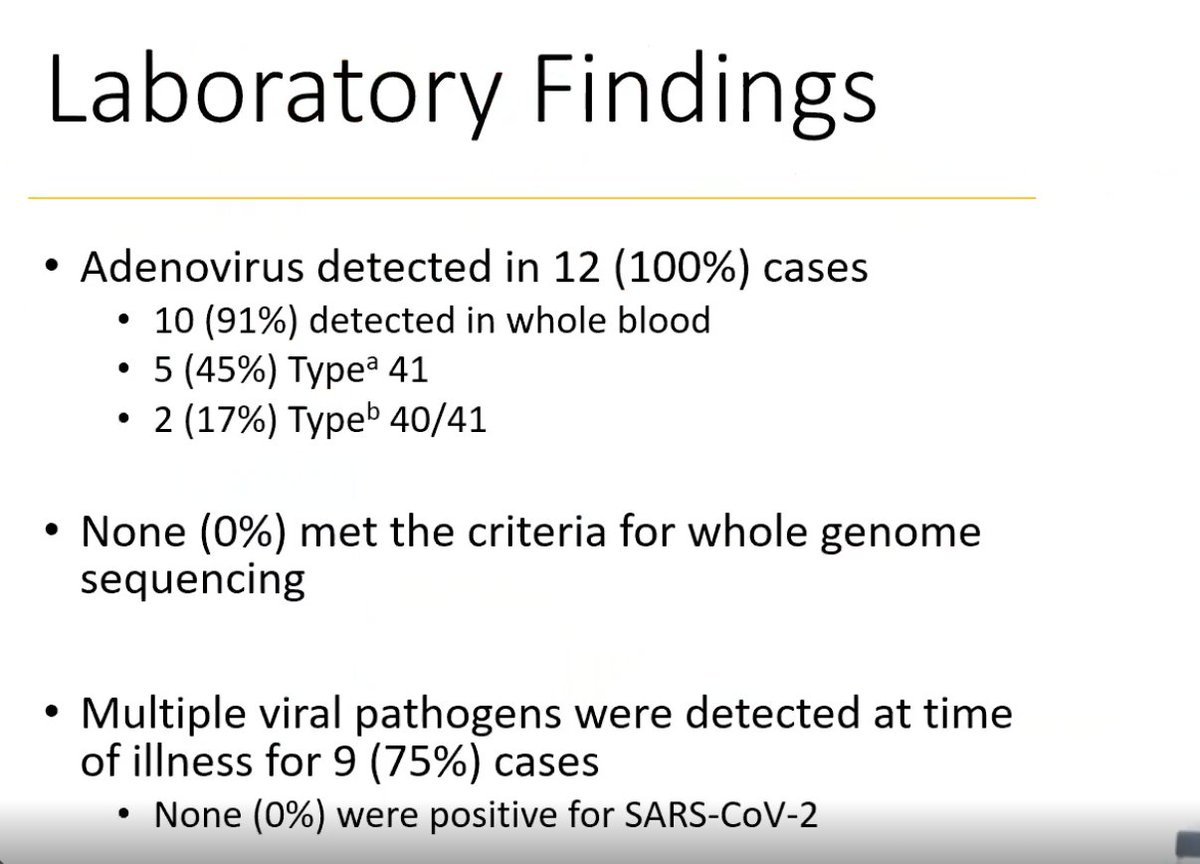
From an epidemiological perspective it's hard to think about what criteria for causality are being met here. As the clinicians describe, there isn't even specificity, given 75% of patients in one cohort had more than one virus on testing. And the Advs weren't even the same type! 
I know I'll be attacked for this thread, but this sort of groupthink in clinical medicine is worrying. Yes, I know these are difficult decisions to make because the stakes are high- but that's exactly why it's important to apply basic principles of clinical diagnostic work
And to me, these don't meet that standard. Nor do they meet the standards of any epidemiological investigation or criteria for causality. And it's astonishing to me that the most plausible cause *still* hasn't been investigated despite so much time gone by.
This is the really key part for me. We've had loads of tests done in different centres across the world- down to metagenomics and what not. Why don't we have COVID-19 serology- perhaps one of the 1st differentials that should've been considered here? I just don't get it.
And getting this right is vitally important. What if this is something that was post-infectious, and auto-inflammatory, and would benefit from steroid treatment? What if some children would be saved a transplant with the right treatment? So rapid assessment for this is vital.
If you're attacking me-please engage on the evidence, and justify how a clinical diagnosis of Adv can be made in this case, when the key diagnostic criterion isn't met. And how a patient can be treated without. And why after wks & wks we still don't have covid serologies for most
I mean even if Adv is playing a role here, isn't it more likely this is still a post-infectious or inflammatory response, given there is no virus in the liver? Shouldn't the treatment be tailored to that?
For those interested in watching:
emergency.cdc.gov/coca/calls/202…
emergency.cdc.gov/coca/calls/202…
• • •
Missing some Tweet in this thread? You can try to
force a refresh