I helped work on this paper on #LongCovid clusters with N3C. It's based on EHR data, which is very biased in Long Covid for multiple reasons, but it's a start. I'd like to see more research factoring in common diagnoses of ME/CFS & dysautonomia.
1/
medrxiv.org/content/10.110…
1/
medrxiv.org/content/10.110…

EHR data is biased towards documented cases, which means:
-more severe/hospitalized cases
-those with access to healthcare
-more respiratory-focused findings (the neurological findings are conspicuously sparse)
2/
-more severe/hospitalized cases
-those with access to healthcare
-more respiratory-focused findings (the neurological findings are conspicuously sparse)
2/
Common symptoms/conditions that clinicians are unfamiliar with - like ME/CFS, post-exertional malaise, dysautonomia - don’t get documented.
Very, very few LC symptoms are documented - only a few ever get written down.
3/
Very, very few LC symptoms are documented - only a few ever get written down.
3/
When doctors don't recognize an illness (esp for neuro or atypical COVID manifestations), they disproportionately diagnose mental health issues instead - that results in an overdiagnosis of anxiety/depression.
4/
4/
So it's very hard to work with EHR data and should be interpreted with those biases in mind. But the team did a good job given the many obstacles they're working with!
5/
5/
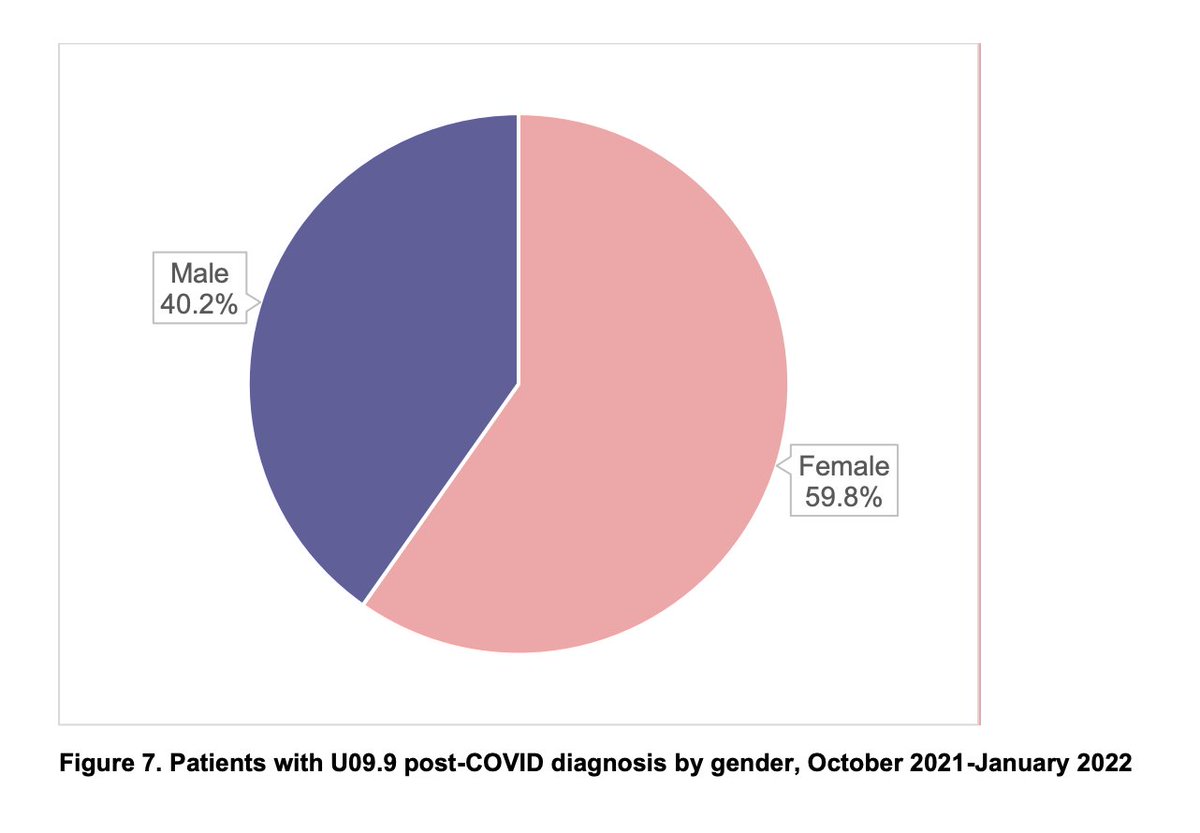
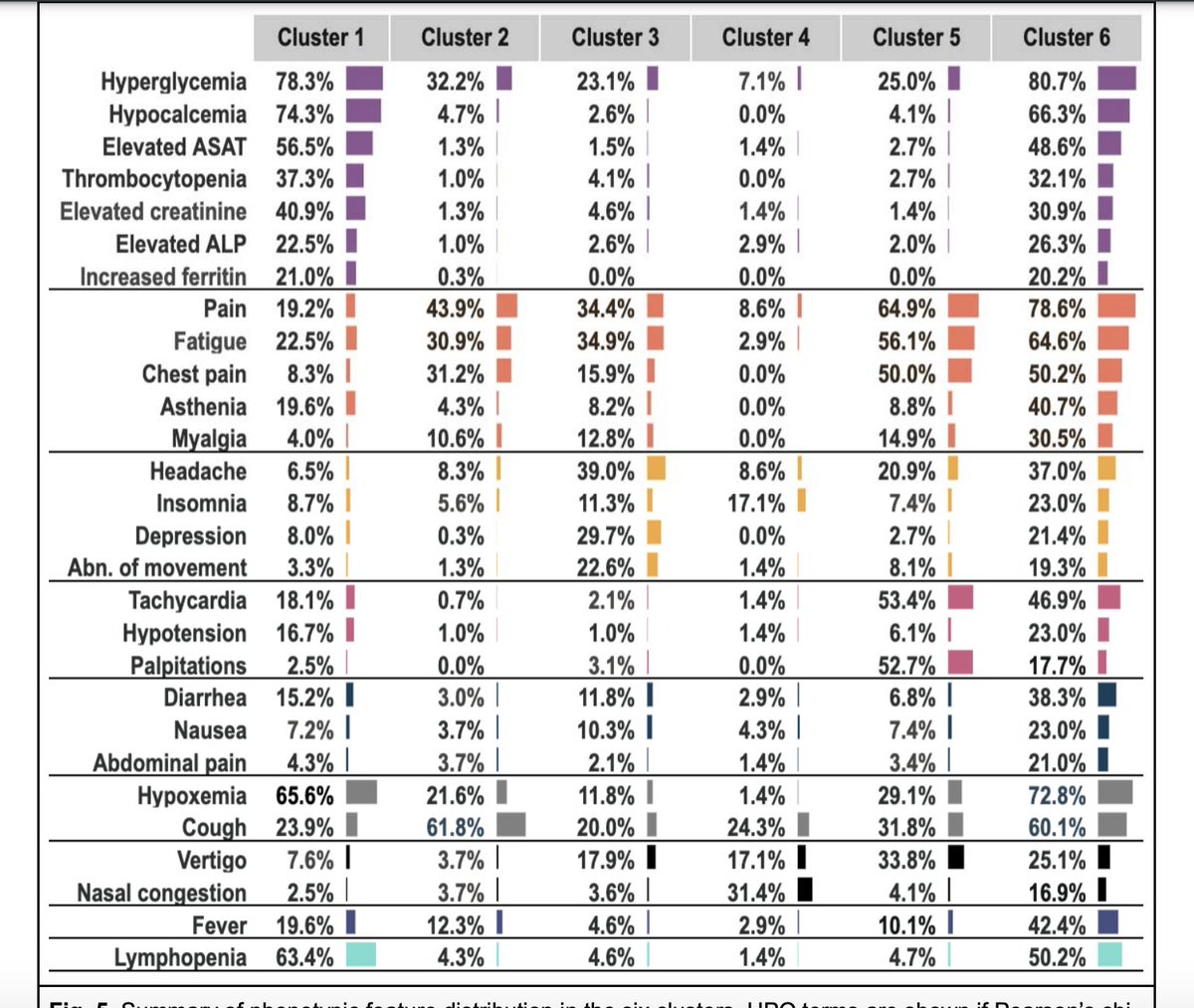
A few things that stick out to me - Cluster 5 could be a dysautonomia/POTS cohort, with lots of tachycardia but low hospitalization, & disproportionately female. Cluster 3 could include ME/CFS folks. Both clusters had high hyperglycemia & importantly didn't have high ferritin. 6/
• • •
Missing some Tweet in this thread? You can try to
force a refresh