
Ever wondered how MR Spectroscopy (MRS) is acquired & how to interpret it? Have you ever come across funky looking zigzag graph with MRI & scratched your head?
If interested in learning BASICS of MRS, follow this 🧵
MRS for non-radiologists
#EmoryNCCTweetorials @MedTweetorials
If interested in learning BASICS of MRS, follow this 🧵
MRS for non-radiologists
#EmoryNCCTweetorials @MedTweetorials

First available since 1980, 1H-MRS is noninvasive technique uses proton signals to determine relative concentrations of tissue metabolites & thereby acquiring data about chemical composition of a tissue.
13C MRS
23Na MRS(neurocognitive,brain tumor research)
31P MRS(🫀&💪🏻research)
13C MRS
23Na MRS(neurocognitive,brain tumor research)
31P MRS(🫀&💪🏻research)
1H-MRS:
-Most widely used
-Performed on 1.5, 3 & 7 T
-Only adds 5-10 min of exam⏰
So why not do it with every MRI?
-Limited value &⬇️specificity
-Most of the time,history & MRI is just enough
-Adding 5-10 mins for every MRI⬇️productivity w/o significant gain in diagnostic yield
-Most widely used
-Performed on 1.5, 3 & 7 T
-Only adds 5-10 min of exam⏰
So why not do it with every MRI?
-Limited value &⬇️specificity
-Most of the time,history & MRI is just enough
-Adding 5-10 mins for every MRI⬇️productivity w/o significant gain in diagnostic yield
That being said, on the verse side, MRS has capability of detecting abnormality even when MRI sequences appear normal - e.g. leukodystrophies / mitochondrial disorders in children, where early WM changes are barely appreciated but MRS can detect it with a reasonable accuracy.
Purpose:
-ID tissue composition in Region of Interest indicated by Voxel (3D;like Pixel for 2D)
-Differentiate between different pathologies based on tissue composition when MRI is similar appearing like High-low grade glioma/metastasis/abscess/radiation necrosis/tumor recurrence
-ID tissue composition in Region of Interest indicated by Voxel (3D;like Pixel for 2D)
-Differentiate between different pathologies based on tissue composition when MRI is similar appearing like High-low grade glioma/metastasis/abscess/radiation necrosis/tumor recurrence
This is what a spectrogram looks like.
Components:
X axis=resonance frequency of metabolite (ppm)
Y Axis=Height of molecule peak depends upon concentration and available 1H
AUC=concentration of metabolite
Right side boxes indicate the Voxel,from which the spectrogram is obtained
Components:
X axis=resonance frequency of metabolite (ppm)
Y Axis=Height of molecule peak depends upon concentration and available 1H
AUC=concentration of metabolite
Right side boxes indicate the Voxel,from which the spectrogram is obtained

MR spectrum=signals from different metabolites ID by unique & highly reproducible frequency distribution
Frequency of metabolite resonance(ppm)=electronic shielding.
Molecules with covalent bonding are coupled and results in doublet peak. E.g.Lactate,Creatinine,Alanine,Lipid.
Frequency of metabolite resonance(ppm)=electronic shielding.
Molecules with covalent bonding are coupled and results in doublet peak. E.g.Lactate,Creatinine,Alanine,Lipid.
Acquisition:
Generally 3 RF pulses are used at 90, 180 and 180 degree in orthogonal planes f/b listening to the signals (TE on x axis) due to Free Induction Decay (y axis)👉🏻Fourier transform👉🏻spectrogram
You can👂signals at any time after beginning of decay which determines 📈
Generally 3 RF pulses are used at 90, 180 and 180 degree in orthogonal planes f/b listening to the signals (TE on x axis) due to Free Induction Decay (y axis)👉🏻Fourier transform👉🏻spectrogram
You can👂signals at any time after beginning of decay which determines 📈

TE=Echo time
Shorter TE=⬇️Free induction decay👉🏻⬆️signal heard.
Short TE=20-40 ms-shows more metabolites but has fluctuating baseline.
Intermediate 135-144 & very long 270-288)-better baseline but shows less metabolites - Cho, Cr, NAA but does not show Myoinositol, GLX & lipids
Shorter TE=⬇️Free induction decay👉🏻⬆️signal heard.
Short TE=20-40 ms-shows more metabolites but has fluctuating baseline.
Intermediate 135-144 & very long 270-288)-better baseline but shows less metabolites - Cho, Cr, NAA but does not show Myoinositol, GLX & lipids
TE matters:
Here is the spectrum form same voxel at different TE.
Short TE=more metabolites but fluctuating baseline, artifactual ⬆️of NAA due to overlap with elevated Glx peak
Longer TE=flatter baseline but less number of metabolites seen, artifactual ⬆️in Cho peak
21215455
Here is the spectrum form same voxel at different TE.
Short TE=more metabolites but fluctuating baseline, artifactual ⬆️of NAA due to overlap with elevated Glx peak
Longer TE=flatter baseline but less number of metabolites seen, artifactual ⬆️in Cho peak
21215455

Magnet strength matters:
⬆️magnet strength has better defined peaks and low signal to noise ratio, gives better diagnostic yield.
Below is comparison b/w 1.5T & 3T
So if you want to see more metabolites with better signal to noise ratio, go for 3T and short TE.
16731366
⬆️magnet strength has better defined peaks and low signal to noise ratio, gives better diagnostic yield.
Below is comparison b/w 1.5T & 3T
So if you want to see more metabolites with better signal to noise ratio, go for 3T and short TE.
16731366

Types of MRS:
-Single voxel(PRESS)
-Multi voxel(MRSI/CSI)
Which technique to use?
It depends upon what is the purpose of spectroscopy in that particular patient.
Single-Identify metabolites in small area for diagnosis
Multi-Compare metabolites over larger area for comparison
-Single voxel(PRESS)
-Multi voxel(MRSI/CSI)
Which technique to use?
It depends upon what is the purpose of spectroscopy in that particular patient.
Single-Identify metabolites in small area for diagnosis
Multi-Compare metabolites over larger area for comparison
Single voxel (3 dimensional)
Uses 3 orthogonal slice selective pulses to select a signal from particular voxel where they intersect. The rest of the signals are removed.
Typical voxel size is 4-8 cm3
However, single voxel MRS does not provide spatial variation of metabolites
Uses 3 orthogonal slice selective pulses to select a signal from particular voxel where they intersect. The rest of the signals are removed.
Typical voxel size is 4-8 cm3
However, single voxel MRS does not provide spatial variation of metabolites

Multi voxel (2 dimensional)
Signal extraction of restricted region using PRESS sequence in 2 dimensions instead of 3.
Hence,you get a plate of voxels(think of it as flattened cube) 👉🏻 used to extract data of each metabolite to create color coded graphs based upon concentration
Signal extraction of restricted region using PRESS sequence in 2 dimensions instead of 3.
Hence,you get a plate of voxels(think of it as flattened cube) 👉🏻 used to extract data of each metabolite to create color coded graphs based upon concentration


Why not get Multi-voxel when you can get more info?
Most of the times single-voxel is sufficient to make diagnosis
Multi-voxel takes longer⏰ to acquire
Multi-voxel MRS is more helpful when one wants to know proliferating part of tumor or differentiating tumor v/s recurrence
Most of the times single-voxel is sufficient to make diagnosis
Multi-voxel takes longer⏰ to acquire
Multi-voxel MRS is more helpful when one wants to know proliferating part of tumor or differentiating tumor v/s recurrence
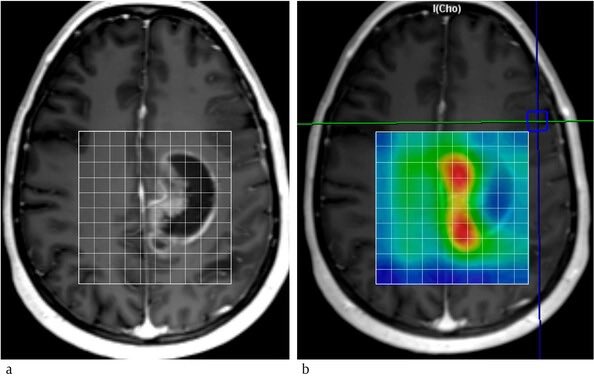
E.g. look at the scan below, on T1+C image, one can’t say what is the active growing part of the mass.
But multi-voxel MRS for Choline reveals red areas with ⬆️choline=indicating rapid proliferation.
T1 hypo intense area is probably the least proliferative, necrotic part.
But multi-voxel MRS for Choline reveals red areas with ⬆️choline=indicating rapid proliferation.
T1 hypo intense area is probably the least proliferative, necrotic part.
CAUTION⚠️
You must suppress Water to see rest of the metabolites
If not👉🏻significantly dwarf other molecular peaks which we are interested in due to ⬆️⬆️concentration of water
Metabolites you can’t see with MRS-Dopamine,Serotonin & Ach- Conc <0.1 mmol/L & Proteins and enzymes
You must suppress Water to see rest of the metabolites
If not👉🏻significantly dwarf other molecular peaks which we are interested in due to ⬆️⬆️concentration of water
Metabolites you can’t see with MRS-Dopamine,Serotonin & Ach- Conc <0.1 mmol/L & Proteins and enzymes

Spectrogram w/o water suppression:
Water resonates at 4.7 ppm and it is in the highest concentration👉🏻tallest peak👉🏻making other metabolite non-recognizable.
Poor water suppression is also suboptimal.
Look at the spectrogram below.
Source: @Radiopaedia
Water resonates at 4.7 ppm and it is in the highest concentration👉🏻tallest peak👉🏻making other metabolite non-recognizable.
Poor water suppression is also suboptimal.
Look at the spectrogram below.
Source: @Radiopaedia

Now the most important, Learning metabolites:
-ID metabolite based on resonance frequency on x-axis (ppm)
-look at the height & shape of peak
-based on overall appearance of different metabolite peaks, differentiate underlying tissue
Here’s the table to remember for metabolites
-ID metabolite based on resonance frequency on x-axis (ppm)
-look at the height & shape of peak
-based on overall appearance of different metabolite peaks, differentiate underlying tissue
Here’s the table to remember for metabolites

Pitfalls:
-Lactate doublet is inverted w/ long TE
-Alanine doublet can be obscured by Lactate👉🏻alanine-specific for meningioma
-Glx can ⬆️NAA falsely at short TE. Compare w/ long TE NAA bcz Glx not seen on long TE
-Unlike Lactate, Lipid doublet doesn’t get inverted at long TE.
-Lactate doublet is inverted w/ long TE
-Alanine doublet can be obscured by Lactate👉🏻alanine-specific for meningioma
-Glx can ⬆️NAA falsely at short TE. Compare w/ long TE NAA bcz Glx not seen on long TE
-Unlike Lactate, Lipid doublet doesn’t get inverted at long TE.



Voxel Location matters:
Spectrogram can look slightly different based upon the location.
More gray matter-⬆️ Cho and Cr, ⬇️NAA
More white matter-⬆️NAA
See below, examples of spectrogram from the same patient with different locations.
Spectrogram can look slightly different based upon the location.
More gray matter-⬆️ Cho and Cr, ⬇️NAA
More white matter-⬆️NAA
See below, examples of spectrogram from the same patient with different locations.

MRS ratios:
Sometimes, ratios of various metabolites is used rather than absolute concentrations.
Helpful in differentiating from low to high grade glioma
-NAA/Cr(abN <1.6)=viability of the tissue
-Cho/Cr (abN >1.5)= indicates cellular proliferation, used to grade neoplasms.
Sometimes, ratios of various metabolites is used rather than absolute concentrations.
Helpful in differentiating from low to high grade glioma
-NAA/Cr(abN <1.6)=viability of the tissue
-Cho/Cr (abN >1.5)= indicates cellular proliferation, used to grade neoplasms.
Cho/NAA(N=0.6) >sensitive and specific than NAA/Cr & Cho/Cr ratio to differentiate gliomas
Hunter’s angle(N~45):straight line drawn through all 3 major peaks (Cho,Cr,NAA) & its angle w/ horizontal plane is called HA
Reversed angle seen in tumors,radiation necrosis, abscess etc.
Hunter’s angle(N~45):straight line drawn through all 3 major peaks (Cho,Cr,NAA) & its angle w/ horizontal plane is called HA
Reversed angle seen in tumors,radiation necrosis, abscess etc.


Take 🏠:
-Identify single / multi voxel
-look at 🧲 strength
-look at TE-short/long
-look at location of voxel & normal spectrogram for that location
-be aware of pitfalls listed before
-ID metabolites & concentration
-look at history, MRI and at last MRS, not reverse.
-Identify single / multi voxel
-look at 🧲 strength
-look at TE-short/long
-look at location of voxel & normal spectrogram for that location
-be aware of pitfalls listed before
-ID metabolites & concentration
-look at history, MRI and at last MRS, not reverse.
End of part 1 of this #tweetorial
In the next part, we’ll look at different patterns in different disease process like infection, tumor, demyelination, stroke & arrest & clinical application of MRS on real life scenarios based upon content above.
Till then, stay tuned…
In the next part, we’ll look at different patterns in different disease process like infection, tumor, demyelination, stroke & arrest & clinical application of MRS on real life scenarios based upon content above.
Till then, stay tuned…
@EmoryNeuroCrit @Capt_Ammonia @caseyalbin @CajalButterfly @sigman_md @JimmySuhMD @mallyaa @EricLawson90 @RyanBPetersonMD @teachplaygrub @a_charidimou @ksuchdev @SrinivasMeghana @rohitmarawar @neuro_intensive @drharunyildiz
• • •
Missing some Tweet in this thread? You can try to
force a refresh







