#EULAR2022
IBD management for Rheumatologist
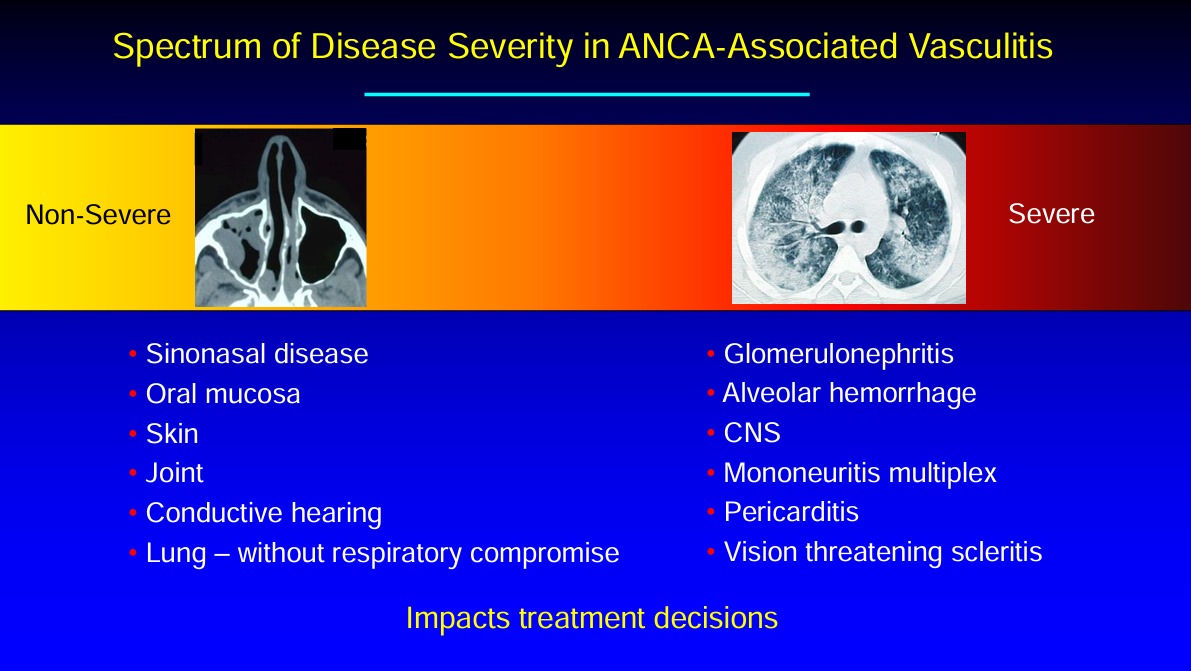
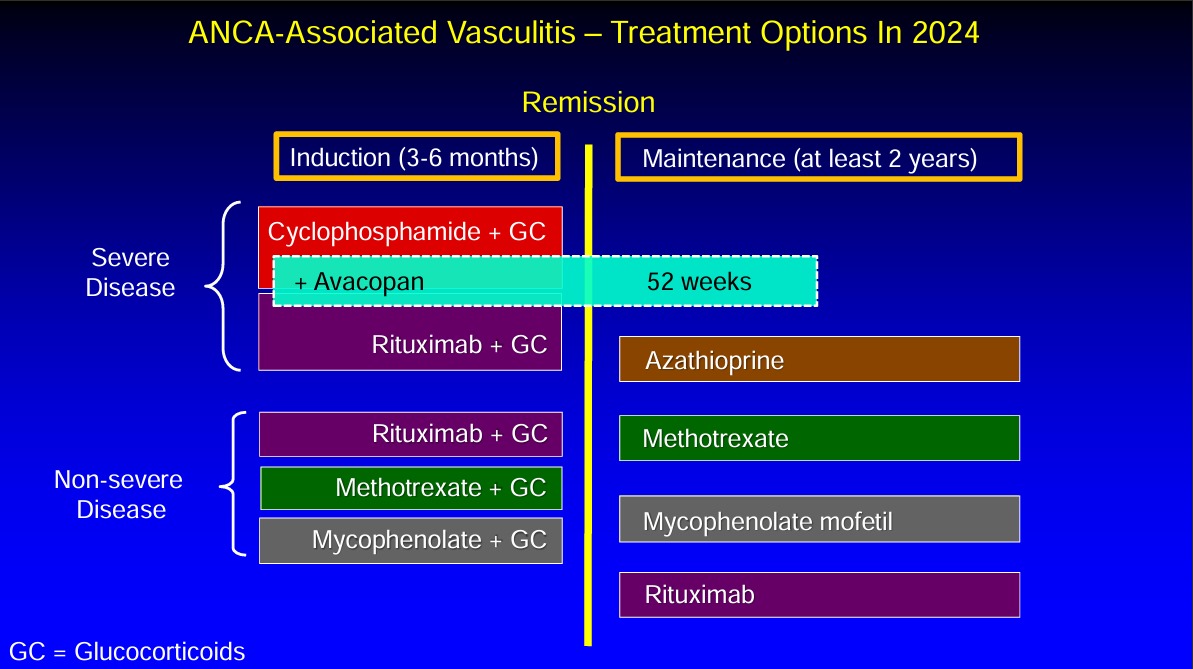
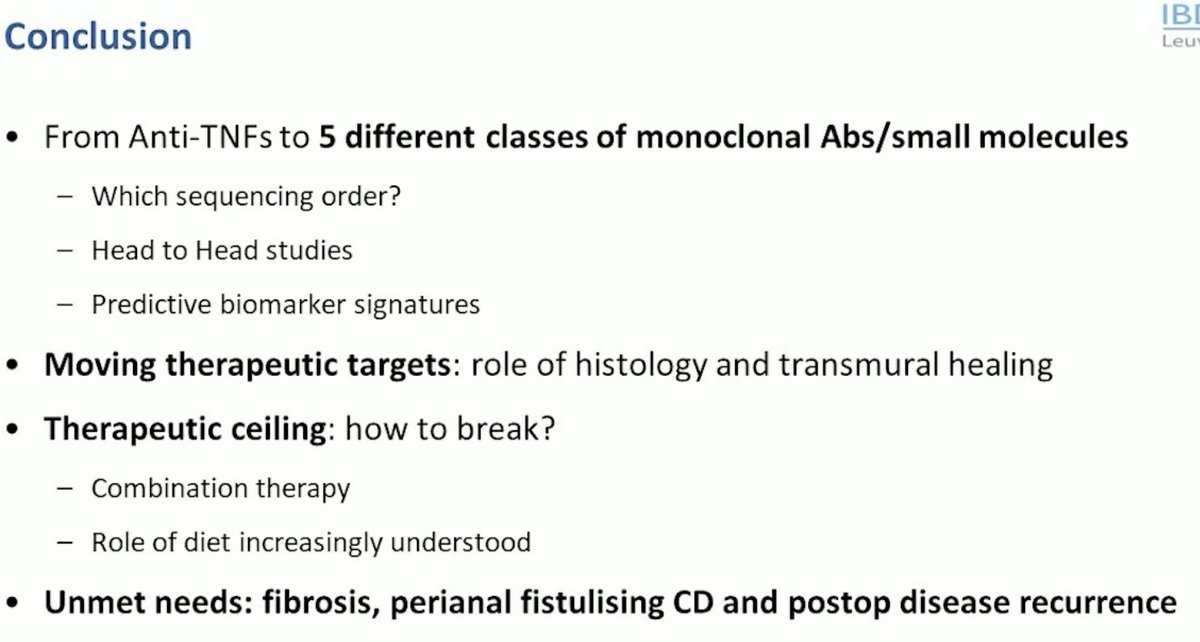
🔎The options have been increasing over the years
🔎Remission rates have still not crossed 30-40% Ballpark
IBD management for Rheumatologist
🔎The options have been increasing over the years
🔎Remission rates have still not crossed 30-40% Ballpark



#EULAR2022
IBD management for Rheumatologist
🔎Target of therapy is
♦️Clinical remission in short term
♦️Histological remission in medium-term
♦️Disease Modification in Long
🔎Histological activity better marker of future Flare
IBD management for Rheumatologist
🔎Target of therapy is
♦️Clinical remission in short term
♦️Histological remission in medium-term
♦️Disease Modification in Long
🔎Histological activity better marker of future Flare



#EULAR2022
IBD management for Rheumatologist
🔎Very Few Head to head trial to decide biologic of choice
🔎 Vedoli>Adali but Ustki=Adali
IBD management for Rheumatologist
🔎Very Few Head to head trial to decide biologic of choice
🔎 Vedoli>Adali but Ustki=Adali



#EULAR2022
IBD management for Rheumatologist
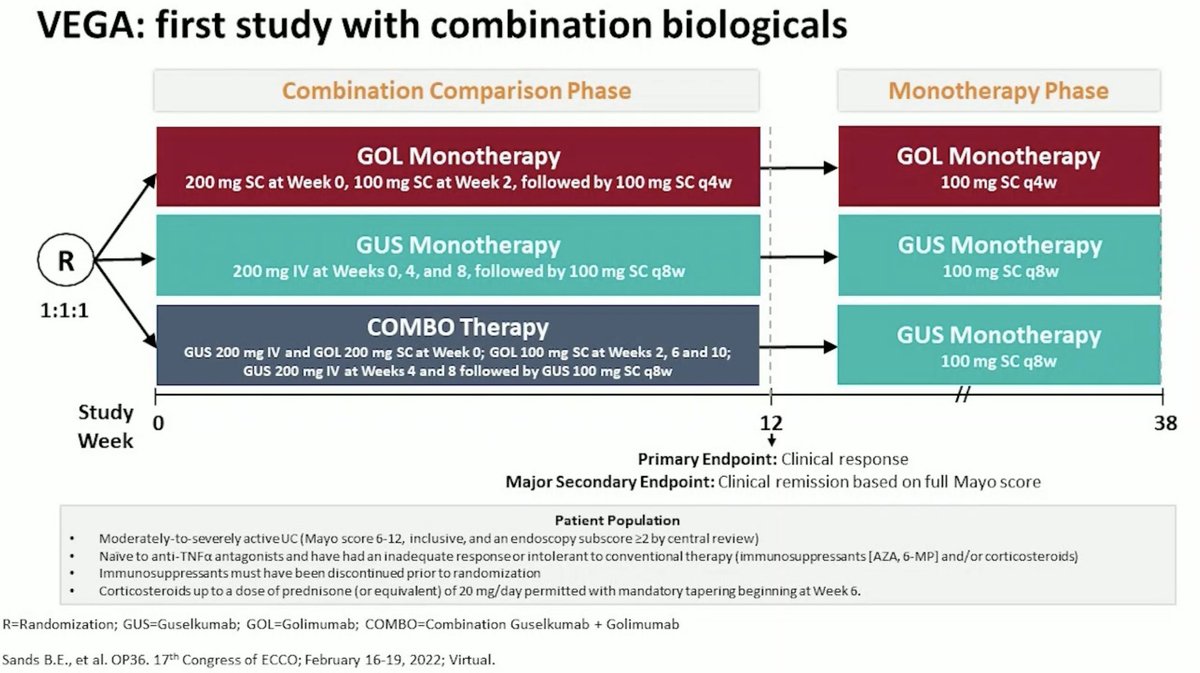
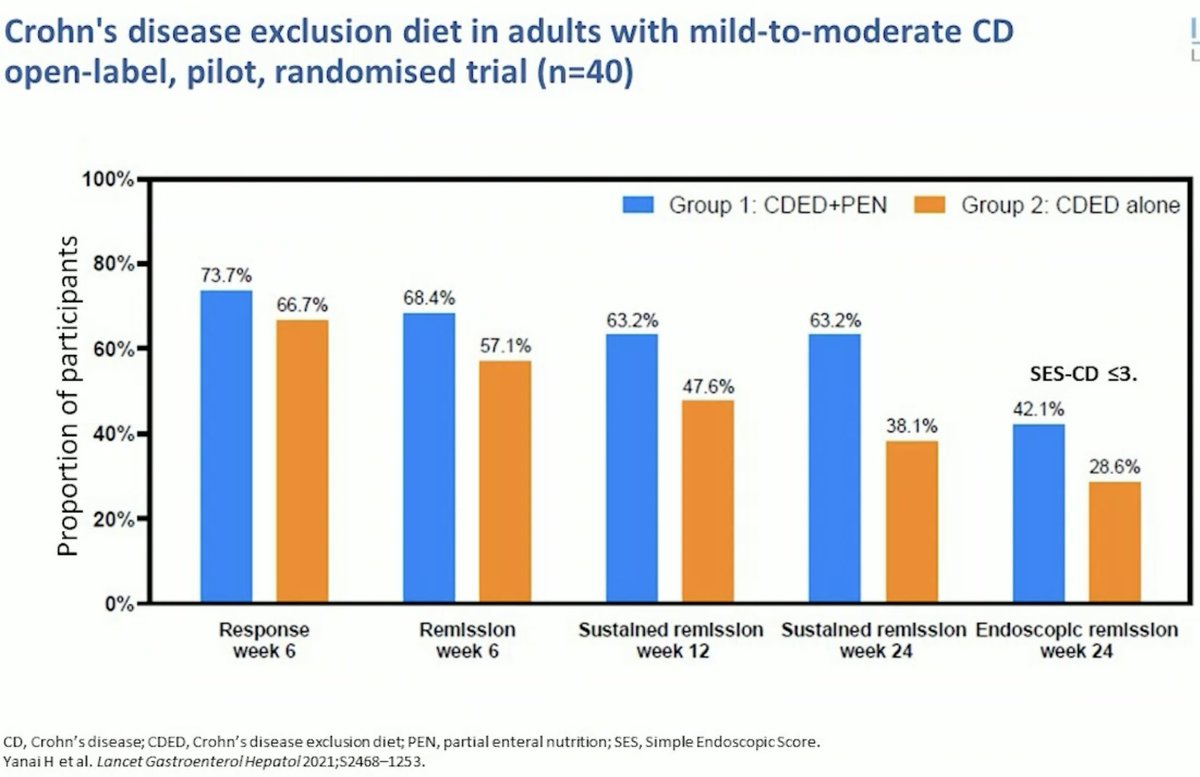
🔎Combination of Biologics or Biologics + DMARDS is way to go for ⬆️ remission rates
🔎 Guselkumab+Golimumab works 👉🏻 intresting 🤔
🔎Ifliximab+AZA also good
IBD management for Rheumatologist
🔎Combination of Biologics or Biologics + DMARDS is way to go for ⬆️ remission rates
🔎 Guselkumab+Golimumab works 👉🏻 intresting 🤔
🔎Ifliximab+AZA also good




#EULAR2022
IBD management for Rheumatologist
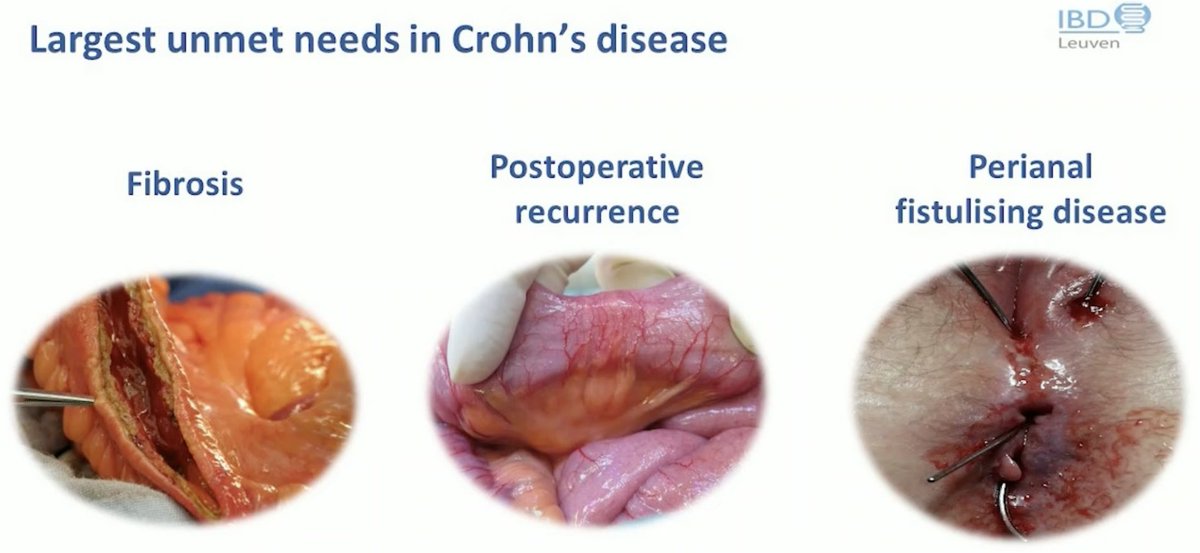
🔎Fibrosis an issue
🔎Post-op flare rates still high (upto 70%)
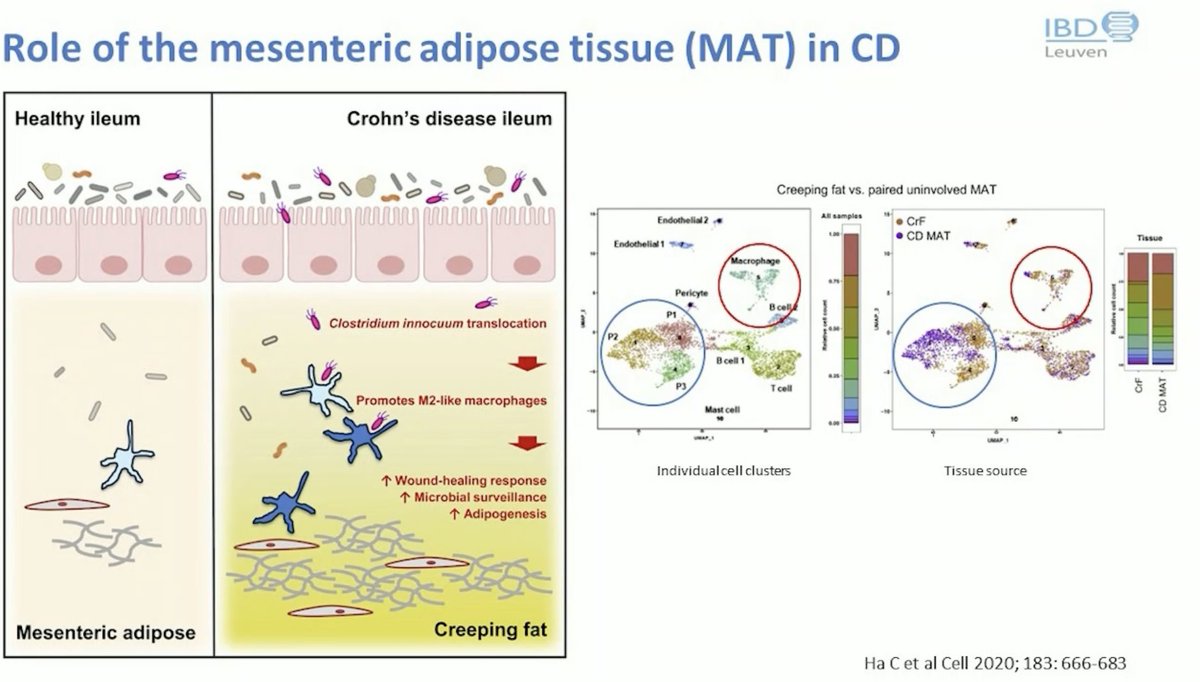
🔎Creeping fat specific for IBD and might start earlier than thought, might be pathological
IBD management for Rheumatologist
🔎Fibrosis an issue
🔎Post-op flare rates still high (upto 70%)
🔎Creeping fat specific for IBD and might start earlier than thought, might be pathological


• • •
Missing some Tweet in this thread? You can try to
force a refresh