Theres a lot of talk about "top 5 or top 10" abstract lists at #asco2022 and a lot of hype.
In this 🧵, I highlight 5 flawed myeloma studies. I mean no offense to the well intentioned investigators, but do this to encourage critical inquiry and debate.
Read on.
#mmsm
In this 🧵, I highlight 5 flawed myeloma studies. I mean no offense to the well intentioned investigators, but do this to encourage critical inquiry and debate.
Read on.
#mmsm
1
meetings.asco.org/abstracts-pres…
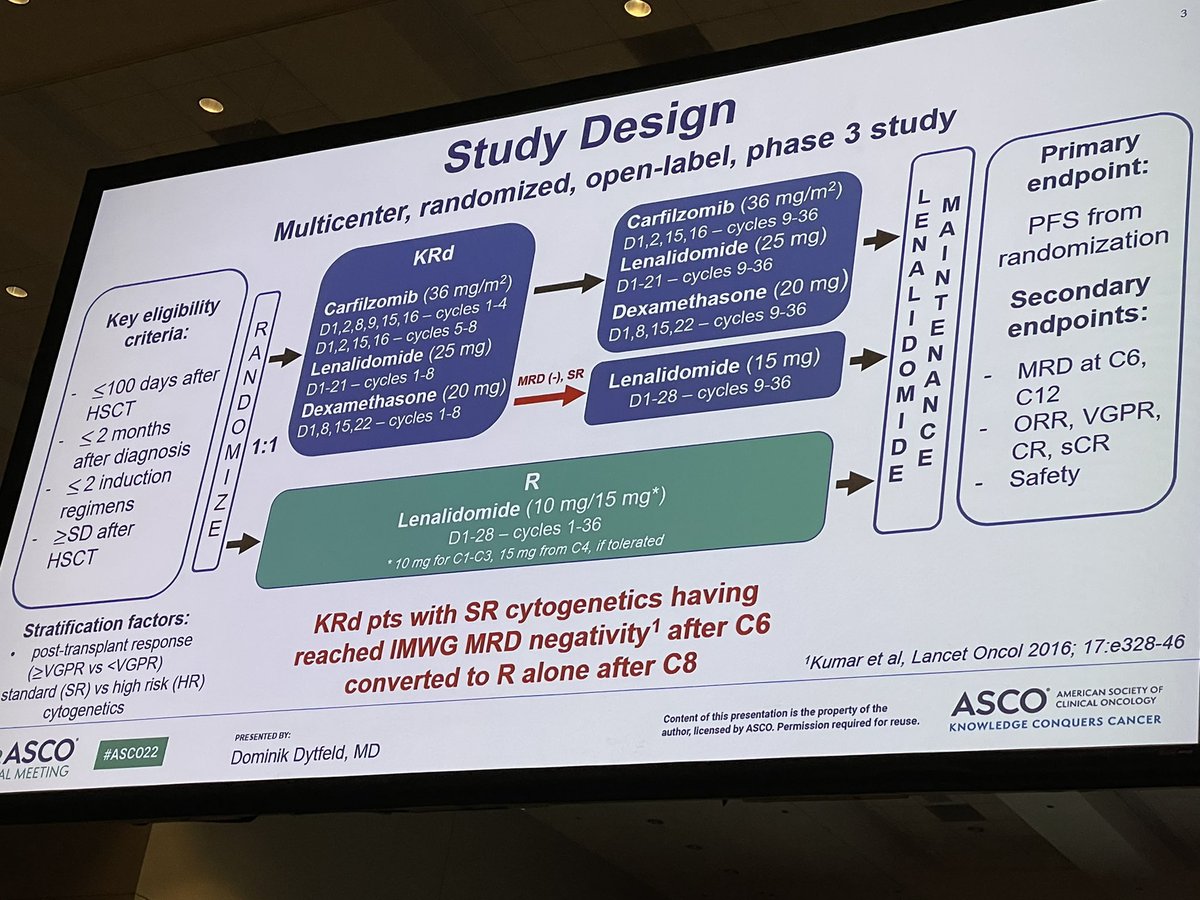
KRD maint vs len maint post auto
Those that were MRD positive paid the "MRD tax" in a big way- 36 months of coming to the infusion center twice a week.
With an endpoint of PFS and comparison of 3 vs 1, result guaranteed.
Wonder what QOL was in K arm?
meetings.asco.org/abstracts-pres…
KRD maint vs len maint post auto
Those that were MRD positive paid the "MRD tax" in a big way- 36 months of coming to the infusion center twice a week.
With an endpoint of PFS and comparison of 3 vs 1, result guaranteed.
Wonder what QOL was in K arm?
2
Dara-RVD for smoldering.
SO PROBLEMATIC.
What does "MRD' negativity even mean in someone with smoldering myeloma? Why should the results of this trial matter any more than the dozens of other duplicative small trials? How can you cure some people who WERE NOT gonna progress?
Dara-RVD for smoldering.
SO PROBLEMATIC.
What does "MRD' negativity even mean in someone with smoldering myeloma? Why should the results of this trial matter any more than the dozens of other duplicative small trials? How can you cure some people who WERE NOT gonna progress?

3
LOCOMOTION
Janssen did not need to do this for teclistamab. It is promising. But they compare different patients in different countries recieving outdated/inferior regimens and then say teclistamab is great. Come on Janssen, do better. "External" controls are so problematic.
LOCOMOTION
Janssen did not need to do this for teclistamab. It is promising. But they compare different patients in different countries recieving outdated/inferior regimens and then say teclistamab is great. Come on Janssen, do better. "External" controls are so problematic.


4) A comparison of teclistamab vs physicians choice in patients who had progressed on trials.
Rather than highlight how good tec is, this draws attention to how bad therapy is for patients once the sponsor is done with the trial.
TECLISTAMAB DOES NOT NEED SUCH COMPARISONS.
Rather than highlight how good tec is, this draws attention to how bad therapy is for patients once the sponsor is done with the trial.
TECLISTAMAB DOES NOT NEED SUCH COMPARISONS.


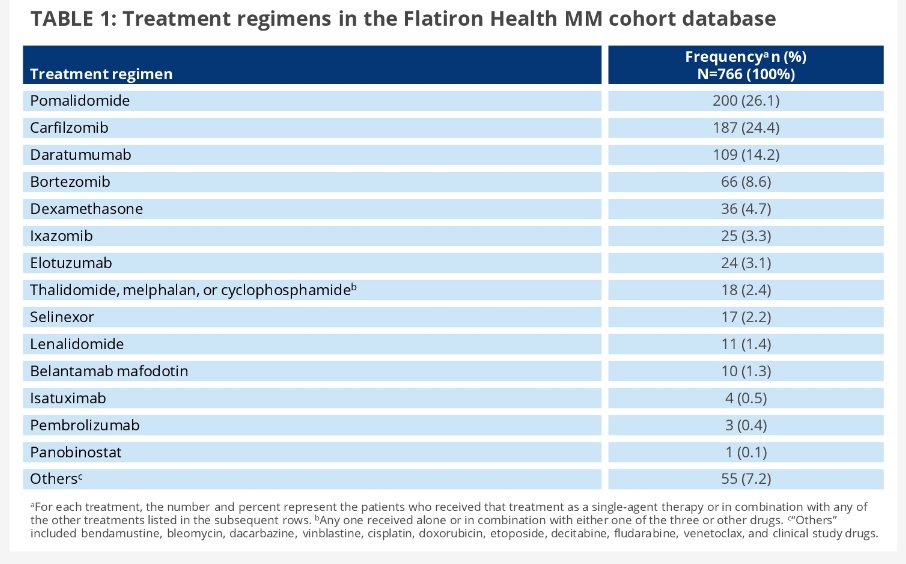
5) Another comparison of teclistamab- this time with flatiron data.
Again, comparing trial patients to those in community from older times (2011 onwards)🙄 receiving outdated tx.
Again, comparing trial patients to those in community from older times (2011 onwards)🙄 receiving outdated tx.

I want us all to ponder how 3 of the limited num of posters were useless teclistamab comparisons that serve only as marketing, and dont help patients or move field forward. Let us all do better. Also dont use KRD maintenance (for stnrd risk), and dont do DRVD for smoldering.
END.
END.
• • •
Missing some Tweet in this thread? You can try to
force a refresh