Important letter published on UK hepatitis cases today on 8 children who were blood DNA adenovirus positive. TLDR:
-6/8 children positive on SARS-CoV-2 serology
-6 needed liver transplants
-Adv not found in *any* of the 6 livers
-treated with cidofovir
🧵
link.springer.com/article/10.100…
-6/8 children positive on SARS-CoV-2 serology
-6 needed liver transplants
-Adv not found in *any* of the 6 livers
-treated with cidofovir
🧵
link.springer.com/article/10.100…
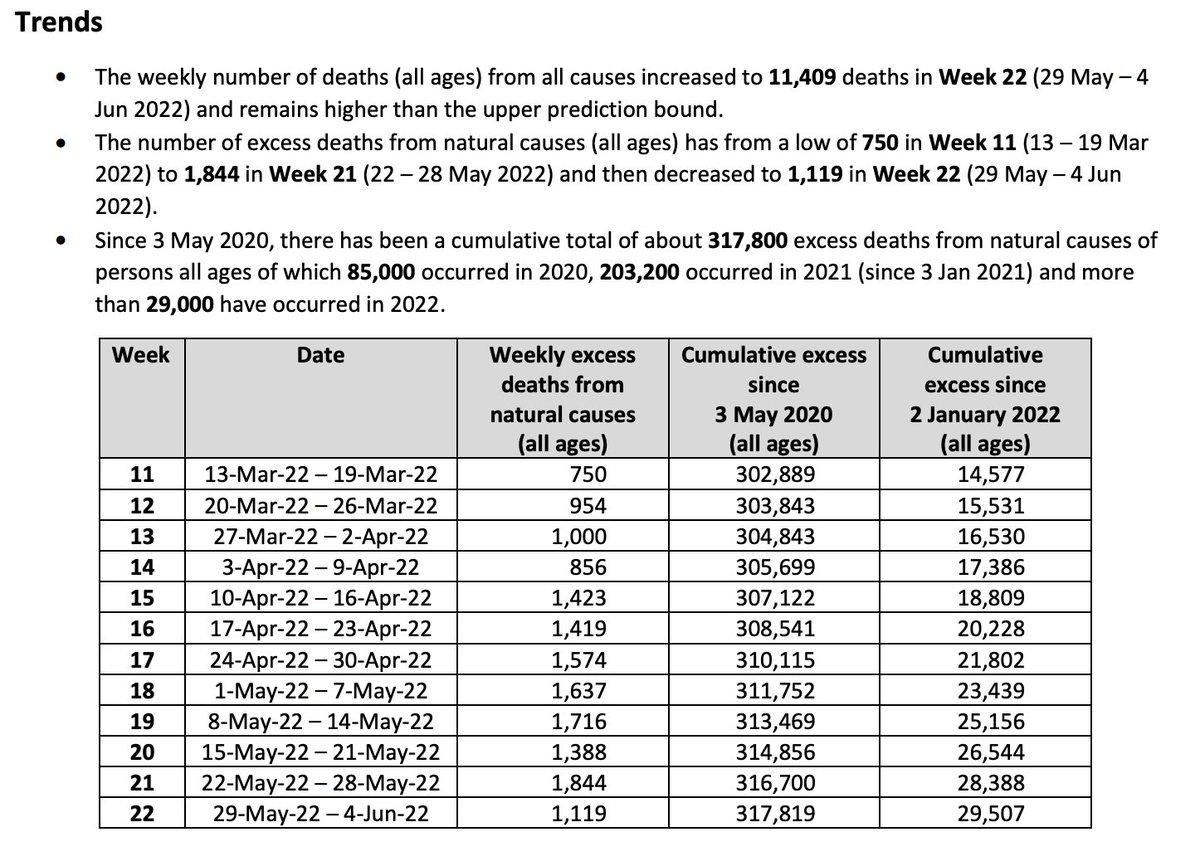
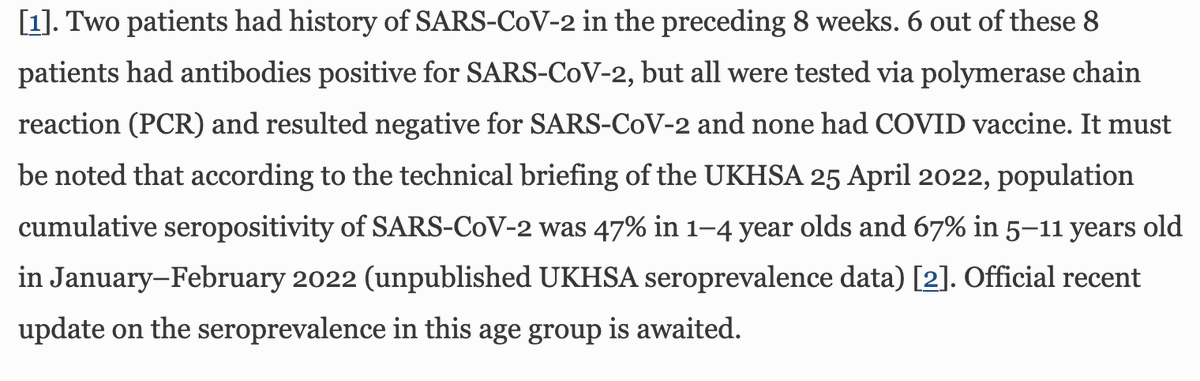
The report clearly shows a 75% seropositivity for SARS-CoV-2 in this small cohort of children - recognising that only 47% of under 5 yr olds were seropositive in the UKHSA April 2022 report - so *much higher* & in line with what we've seen before with PIMS-TS. 
But still seems to bizarrely conclude that this must be adenovirus related. It says that 68% of UK samples had adenovirus in blood (*none* in liver)- and *not even all of these* were the same type of Adenovirus! The most common type was Adv 41 - *never* known to cause hepatitis.

This statement from the authors is quite bizarre. "we didn't find adv in the liver, but this might be because of an abberent immune response"... or maybe it's just *not* adenovirus? Look at the evidence- Adv41 has *never* done this. And it's not even found in the liver.
Even the adenovirus in blood wasn't the same *type* of adenovirus in everyone. And viral levels in blood were so low that it couldn't even be sequenced. By contrast, 75% of children were seropositive for COVID-19 *much* higher than the community rate.
And SARS-CoV-2 is known to cause fulminant hepatitis, and geographical and temporal associations fit- it's very clear that most cases have occurred in places where children were highly infected. Of course, correlation isn't causation, but it's an indicator.
Other countries have not consistently even found adenovirus in blood- suggesting very much that this is a UK association that's likely incidental. Reports from many other countries (e.g. Japan, Austria, some parts of the US) don't show high Adv positivity in cases.
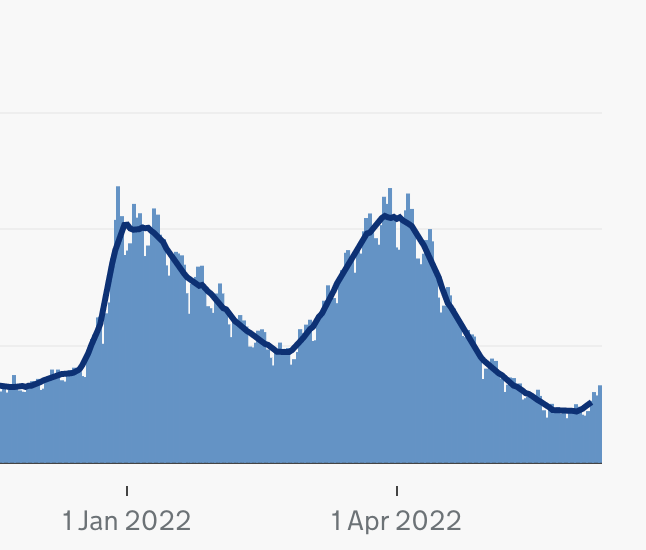
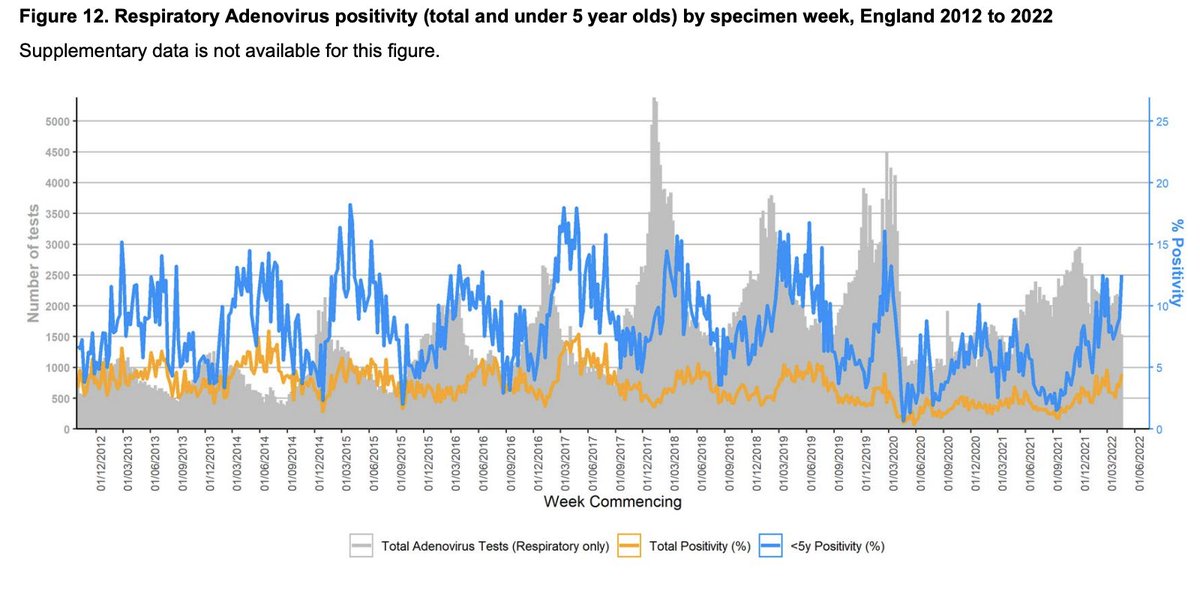
Israel, Austria have already reported that all their cases were post-covid and have been treating with steroids. Plus - adenovirus hasn't even increased in England in line with hepatitis cases. If you look at UKHSA reported adenovirus *positivity* it's entirely flat over time.
If you look at routine surveillance from Wales- that shows the same. What seems to have increased is case ascertainment through increased testing. by contrast ~50% of young children have been infected with SARS-CoV-2 since Dec '21.
This is quite a worrying level of groupthink- where children have been treated with antivirals against a virus that's very likely incidental in this case. Why is this important? Here's why:
If we can prevent even one child needing a transplant, we should. And that means acknowledging that diagnostic criteria for adenovirus were *not met* in these cases. And acknowledging that its very likely groupthink has led to this. We need to do better by these children.
The authors discuss using steroids, but not in the context of SARS-CoV-2 - post-inflammatory response. Why? Isn't this the most obvious potential cause here? Why bring in a virus that's never caused this, is present in extremely low levels in blood & not found in liver!
We just *cannot* justify a diagnosis of Adv hepatitis if it isn't found in the liver. Nor can we ignore that SARS-CoV-2 is known to do this. And children in other countries have responded well to steroids. Let's learn from them & do right by these children.
What's happening now reminds me of the sort of groupthink that led to 'herd immunity' narratives even among well-meaning scientists in March 2020, and a late lockdown that cost tens of thousands of lives. Let's never let that sort of groupthink affect how we act ever again.
I never expected to be living in a time where clinicians in some parts of the world would be diagnosing and treating something in seriously ill children that isn't backed up by basic diagnostic criteria - when there is a much more plausible explanation - that's being ignored.
It's terrifying to think this is happening. These are children. Very very very sick children. Mistakes here can cost lives - or at the very least change lives permanently. Please please rethink this. What we're doing doesn't make sense. Better to acknowledge this now.
And again, where is the serology for the rest of the patients in the UK? Can UKHSA please report on this? This could save lives.
When you have two completely different therapies (cidofovir vs steroids) for a serious disease in children being administered in different parts of the world, something has gone badly wrong. We really need to understand what that is, & compare clinical outcomes of patients.
Sorry, want to add that the positive serology is technically 6/7 - because one result was indeterminate. So only *one* was negative. Which means 86% positivity- in a group that generally has a low seroconversion rate. Thanks for pointing this out @CPita3
we wouldn't expect this sort of seroconversion in this age group even with 100% exposure - clearly not only is exposure high here, but seroconversion rate also seems higher- suggesting not only recent infection, but also potent immunological responses.
• • •
Missing some Tweet in this thread? You can try to
force a refresh