Now that the Israel report is out on paeds hepatitis, we're already seeing push back from various scientists/public health officials who have either played a role in pushing the Adv narrative/minimised impact of SARS-CoV-2 on kids. Here're some of the most inspired takes:-
1. The 'but is the Israel study really sound?' takes:
-'they had small numbers. UK have more patients' (no points for guessing why...)
-'yes, all the patients developed hepatitis after COVID & had no evidence of any other virus - but there are no controls so not a rigorous study'
-'they had small numbers. UK have more patients' (no points for guessing why...)
-'yes, all the patients developed hepatitis after COVID & had no evidence of any other virus - but there are no controls so not a rigorous study'
2. The 'Is the Israel study really relevant to us?' takes
-'they didn't have excess hepatitis cases like we do, so it's not the same thing' (again, no points for guessing why we have 'excess cases' of hepatitis in children)
-'they didn't have excess hepatitis cases like we do, so it's not the same thing' (again, no points for guessing why we have 'excess cases' of hepatitis in children)
'Cases are from 2021- so not relevant to us now'...
yes, that's because that's one of the key periods Israel had high infection in children (although still lower than we did in 2022). And they have excellent surveillance, as we've seen from their previous reports on vaccines.
yes, that's because that's one of the key periods Israel had high infection in children (although still lower than we did in 2022). And they have excellent surveillance, as we've seen from their previous reports on vaccines.
3. The 'but it's nothing new' takes
'there's nothing new about this- it's just MIS-C' (this is true, there is nothing novel about this. Other countries had reported hepatitis dominant MIS-C already. So *why* did we consider adenovirus, when we knew this happens with SARS-CoV-2!)'
'there's nothing new about this- it's just MIS-C' (this is true, there is nothing novel about this. Other countries had reported hepatitis dominant MIS-C already. So *why* did we consider adenovirus, when we knew this happens with SARS-CoV-2!)'
4. The 'but even if it's covid, it's still pretty rare' takes
'We accept a level of fulminant hepatitis in children, so what's a few more cases of MIS-C?'
'We accept a level of fulminant hepatitis in children, so what's a few more cases of MIS-C?'
I think I've covered most of what I've seen today, but please feel free to add any I may have missed! I'm sure we'll see more moving forward.
Yes, I forgot this one- thanks for pointing out!
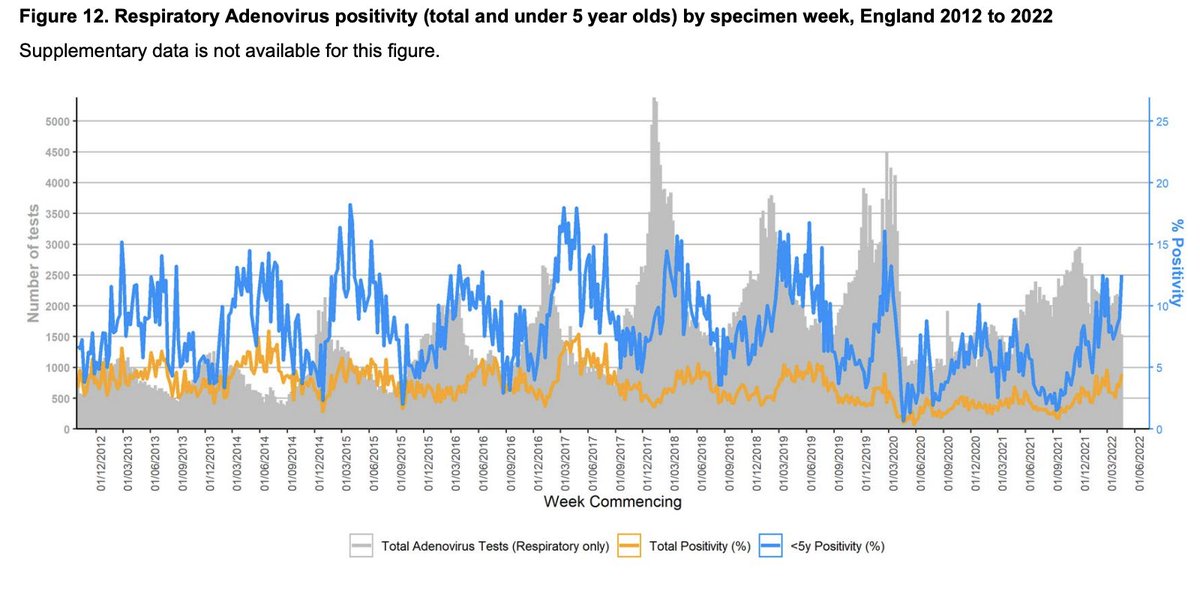
The 'but almost all kids are already infected, so serology is useless' takes (it isn't useless- the April UKHSA report showed ~47% positivity in under 5s- this is expected to be higher now- but not at 100%)
The 'but almost all kids are already infected, so serology is useless' takes (it isn't useless- the April UKHSA report showed ~47% positivity in under 5s- this is expected to be higher now- but not at 100%)
https://twitter.com/Ecole_Oubliee/status/1536092966003015681?s=20&t=PbruF7EXFPJCSAqiPVHTuw
Under 5 comparisons are the most relevant, and the UK recent report showed (6/7) 85% acute hepatitis cases were seropositive, so pretty indicative....
There's more. Time to extend the list-
the 'most cases don't require transplant' take (yup *just* 7-10%)
the 'they got a transplant but didn't die' take (true for many, but transplants require taking immunosuppression for life & are associated with reduced survival long-term)
the 'most cases don't require transplant' take (yup *just* 7-10%)
the 'they got a transplant but didn't die' take (true for many, but transplants require taking immunosuppression for life & are associated with reduced survival long-term)
And then there's the rewriting history:
the 'they didn't say it was adenovirus hepatitis' take (they said it was the most plausible cause, and guidelines were to treat with cidofovir - both in the US and the UK. And they treated for this, not with steroids in most cases)
the 'they didn't say it was adenovirus hepatitis' take (they said it was the most plausible cause, and guidelines were to treat with cidofovir - both in the US and the UK. And they treated for this, not with steroids in most cases)
• • •
Missing some Tweet in this thread? You can try to
force a refresh