
COVID-19: Viral characteristics of BA.4/BA.5 & BA.2.12.1
The newest Omicron variants BA.4 and BA.5 have been spreading around the world and now growing in Canada and the USA. 🧵1/
The newest Omicron variants BA.4 and BA.5 have been spreading around the world and now growing in Canada and the USA. 🧵1/
They appear to have enhanced replication in lung cells compared to BA.2 and is more fusogenic and pathogenic than BA.2 in an animal model ( biorxiv.org/content/10.110… ). 2/
Sato Lab has looked at BA.4, BA.5, and BA.2.12.1 which seem to have an effective reproduction number 1.2x higher than BA.2 so even more transmissible (
https://twitter.com/SystemsVirology/status/1529953265017757696). 3/
Unfortunately neutralization experiments found that BA.4/5 is 2x more resistant than BA.2 to the blood obtained from vaccinated individuals who had a breakthrough infection with BA.1 or BA.2. 4/ 
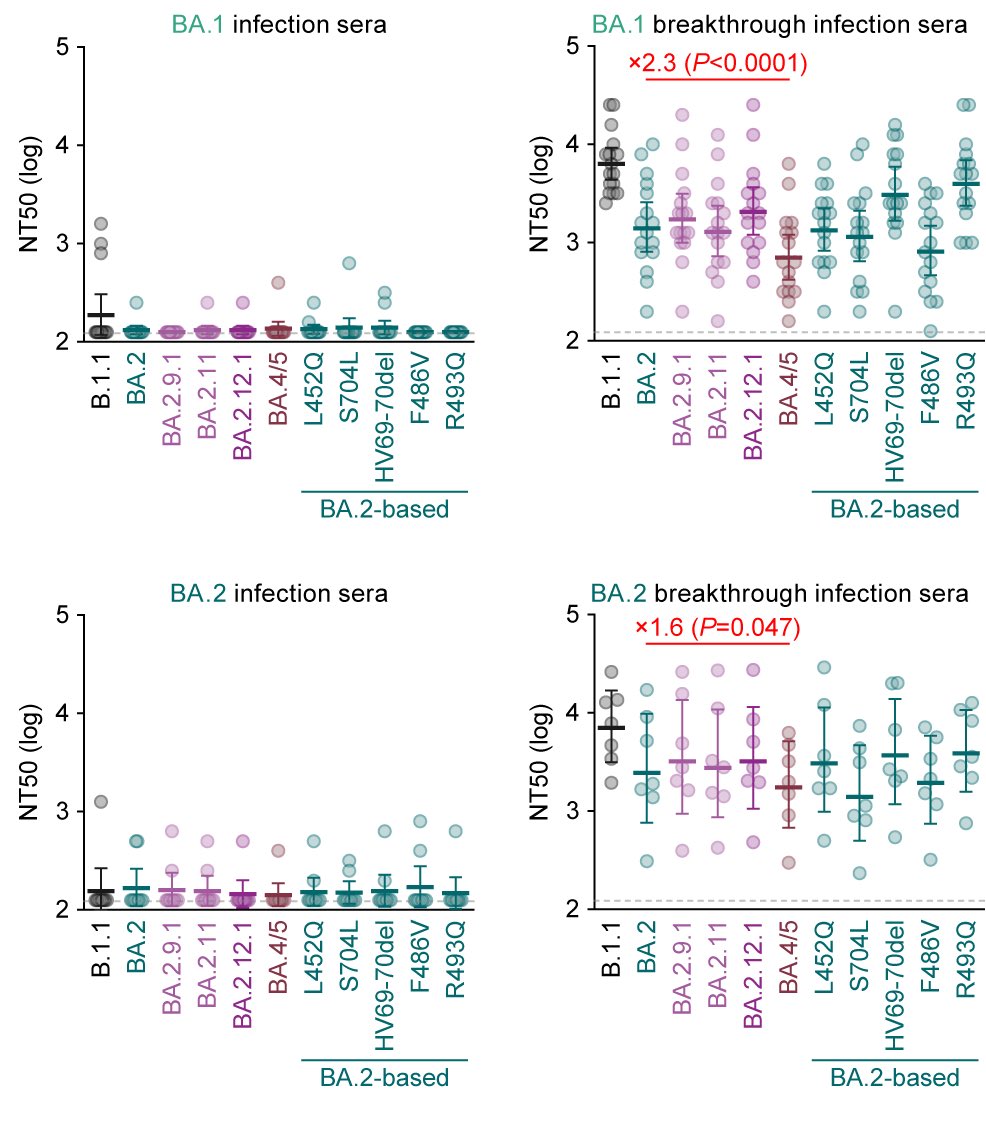
It is also important to note that BA.1 or BA.2 infection in the unvaccinated does *not* induce functional immunity against BA.4/5 so people get all the potential damage from that previous BA.1/BA.2 infection without all the benefits of protection. 5/

The researchers conclude that their investigations suggest that BA.4 and BA.5 have a greater potential global health risk than the original BA.2 variant. 6/
Those are lab results, what about the real world? Portugal has been hit with a BA.5 wave and you can see from the graph that their hospitalization rate spiked significantly, much higher than their Delta wave, despite very high vaccination rates ( ourworldindata.org/explorers/coro… ). 7/

The daily deaths rates from COVID-19 in Portugal have almost matched their BA.1 wave several months ago, significantly higher than the Delta wave and even first wave back in March 2020 before anyone was vaccinated ( ourworldindata.org/explorers/coro… ). 8/

Excess deaths from all causes in Portugal was up 20% in mid-May 2022 ( ourworldindata.org/excess-mortali… ). 9/
South Africa also had a big BA.4/BA.5 wave and they have seen 29,500 excess deaths since January (Omicron wave) with a peak of 1,844 excess deaths/week during the current BA.4/5 wave (
https://twitter.com/dgurdasani1/status/1535710130767110157). 10/
This will be the 3rd wave in the UK within 6 months, and Long COVID is an increasing issue (
https://twitter.com/chrischirp/status/1535280913415913477). It looks like BA.2.12.1, BA.4, and BA.5 are all at similar levels in England right now, which one will win out? 11/
It was BA.5.1 that became dominant in Portugal ( outbreak.info/location-repor… ) and BA.4 that is more prevalent in South Africa ( outbreak.info/location-repor… ). 12/
Hospitalisations are starting to increase in England with a new wave and deaths will likely follow in a few weeks (
https://twitter.com/dgurdasani1/status/1535190012379144192). 13/
Hospital admissions up 17% week-on-week in England, with the fastest increase in the South East which was up 30% and hospital bed occupancy up 11% (
https://twitter.com/COVID19actuary/status/1535279946834354177). 14/
Countries in Europe seem to get COVID-19 waves earlier than we do in Canada, like an early warning system, so we can likely expect similar things here to come. 15/
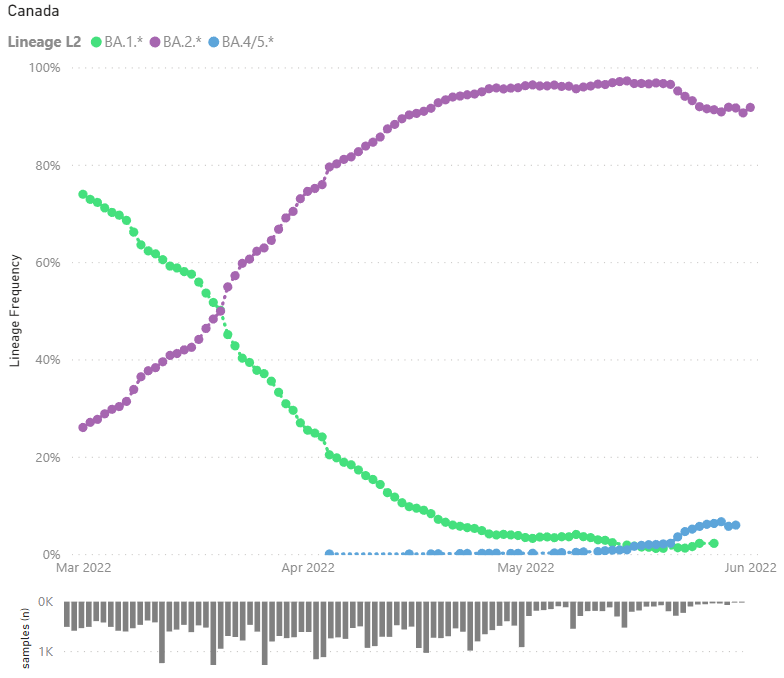
You can see from the graph that BA.4/5 is already here in Canada (blue line) at around 6% and starting to increase ( app.powerbi.com/view?r=eyJrIjo… ). This data was from almost 2 weeks ago so it is likely higher now. 16/
With provinces removing data from their websites and only making updates available once a week, combined with extremely limited PCR testing, it is becoming harder and harder to see what is actually going on in the community and whether new variants of concern are emerging. 17/
What I do know is that despite people claiming Omicron is "mild" and wastewater levels decreasing, Hospitals are still being pushed beyond their limits. 18/
The Children's Hospital in Ottawa is seeing new record levels of patients in its 48-year history and has people waiting in the ER for beds, some for almost 2 days (
https://twitter.com/CHEO/status/1536014654434066432). 19/
The city has also had 528 incidents this year where no ambulances were available, which is more than 10x higher than this time last year (
https://twitter.com/jeffgilchrist/status/1535783757990400000). 20/
A new wave from BA.4/5 while no real efforts were made to improve indoor ventilation and even fewer measures are in place to prevent the transmission of COVID-19 is going to make things even worse. 21/
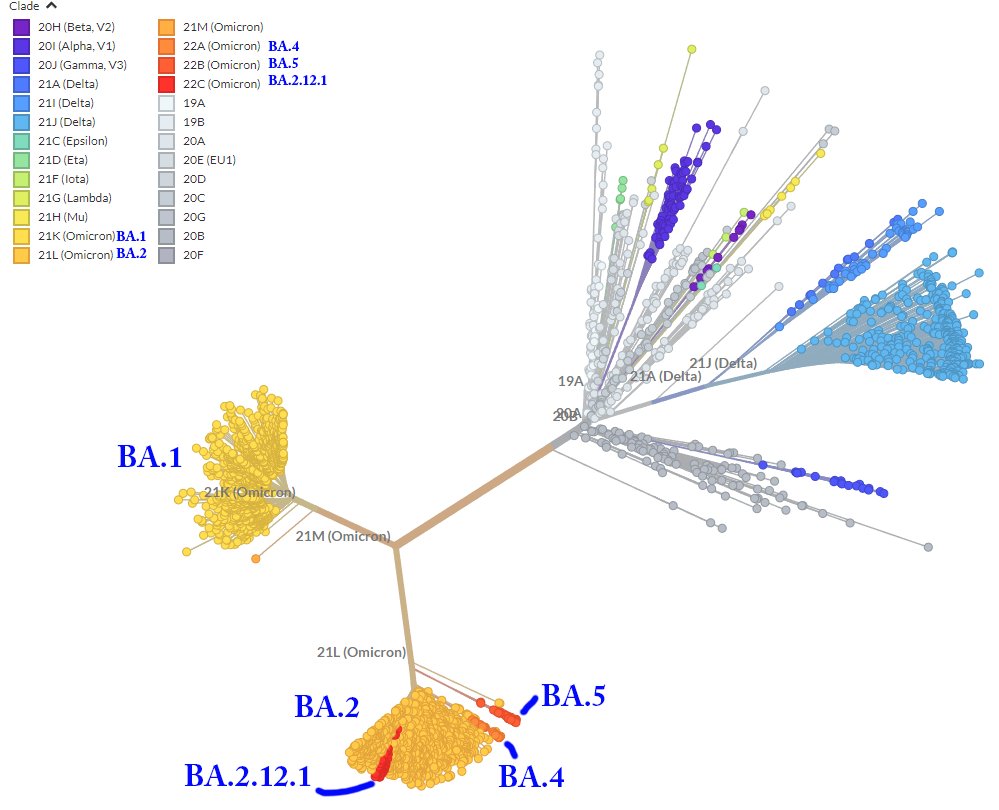
For people who want to see a visual Phylogeny of the variants, I have taken the information from Nextstrain and labelled it. See the original here ( nextstrain.org/ncov/gisaid/gl… ). 22/
• • •
Missing some Tweet in this thread? You can try to
force a refresh






