📌 Tweetorial on Diagnosis & Pathogenesis of IgA Nephropathy (IgAN) based on @goKDIGO webinar by @AgnesFogo & Dr. Jurgen Floege
#IgAN
🔸Interesting fact: IgAN is not a new disease
First known case of IgAN was found in Prince Joseph of Austria (1776-1847)
1/
#IgAN
🔸Interesting fact: IgAN is not a new disease
First known case of IgAN was found in Prince Joseph of Austria (1776-1847)
1/

📌 IgAN is characterized by:
🔸Mesangial immune-complex deposits which sometimes can extend to the capillary loops & sub-endothelial locations
🔸 Dominant IgA deposits compared to the other immunoglobulins
2/
🔸Mesangial immune-complex deposits which sometimes can extend to the capillary loops & sub-endothelial locations
🔸 Dominant IgA deposits compared to the other immunoglobulins
2/

📌 IgA deposits in IgAN are typically polyclonal & lambda is more prominent than kappa
🔸This is thought to represent the mucosal IgA
3/
🔸This is thought to represent the mucosal IgA
3/

📌 IgA deposits can be found in other conditions:
🔸Liver disease, inflammatory bowel disease: IgA is focal, weak
🔸Lupus: IgG is co-dominant, full house pattern is seen
🔸IgA-dominant infection associated GN: +C3, hump-deposits, kappa>>lambda
4/
🔸Liver disease, inflammatory bowel disease: IgA is focal, weak
🔸Lupus: IgG is co-dominant, full house pattern is seen
🔸IgA-dominant infection associated GN: +C3, hump-deposits, kappa>>lambda
4/

📌 IgAN can have a varying expression of kidney injury:
🔸Mesangial proliferation
🔸Endocapillary proliferation
🔸Crescent formation (when GBM breaks -> parietal epithelial cells are exposed to the fibrinoid material in human plasma & they form crescents
5/
🔸Mesangial proliferation
🔸Endocapillary proliferation
🔸Crescent formation (when GBM breaks -> parietal epithelial cells are exposed to the fibrinoid material in human plasma & they form crescents
5/


📌 The Oxford classification of IgAN attempted to define the histological lesions seen on kidney biopsy & examined the clinical outcomes related to these lesions👇🏽
kidney-international.org/article/S0085-…
6/
kidney-international.org/article/S0085-…
6/
📌 Oxford classification of IgAN: the initial biopsy study set included 256 patients but it excluded pts. with:
🔸IgA vasculitis, DM, minimal proteinuria (<0.5 g/d), eGFR <30, rapidly progressive kidney disease, 🔸 Very few patients had crescents
7/
🔸IgA vasculitis, DM, minimal proteinuria (<0.5 g/d), eGFR <30, rapidly progressive kidney disease, 🔸 Very few patients had crescents
7/

📌 Subsequent studies of the Oxford classification of IgAN included a larger number & a broader range of patients (including pts. with crescents)
jasn.asnjournals.org/content/28/2/6…
🔸The following histological lesions appear to correlate w/ clinical outcomes👇🏽
8/
jasn.asnjournals.org/content/28/2/6…
🔸The following histological lesions appear to correlate w/ clinical outcomes👇🏽
8/
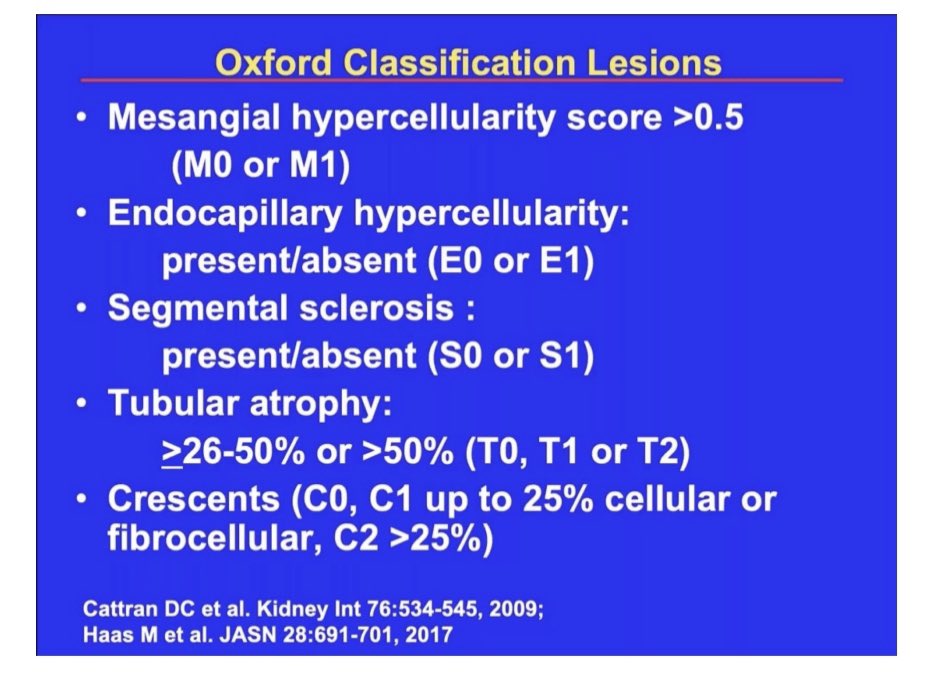

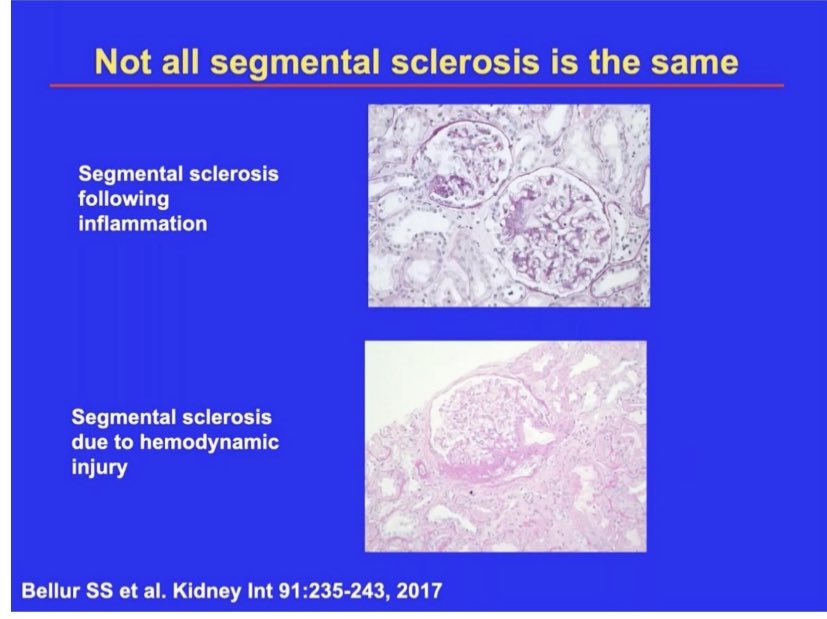
📌 There are some limitations of the Oxford classification of IgAN
🔸Reproducibility of scores at the local pathologist level (M, E lesions)
🔸 May need to differentiate the sclerotic lesions based on the underlying cause: inflammation vs. hemodynamic
9/
🔸Reproducibility of scores at the local pathologist level (M, E lesions)
🔸 May need to differentiate the sclerotic lesions based on the underlying cause: inflammation vs. hemodynamic
9/

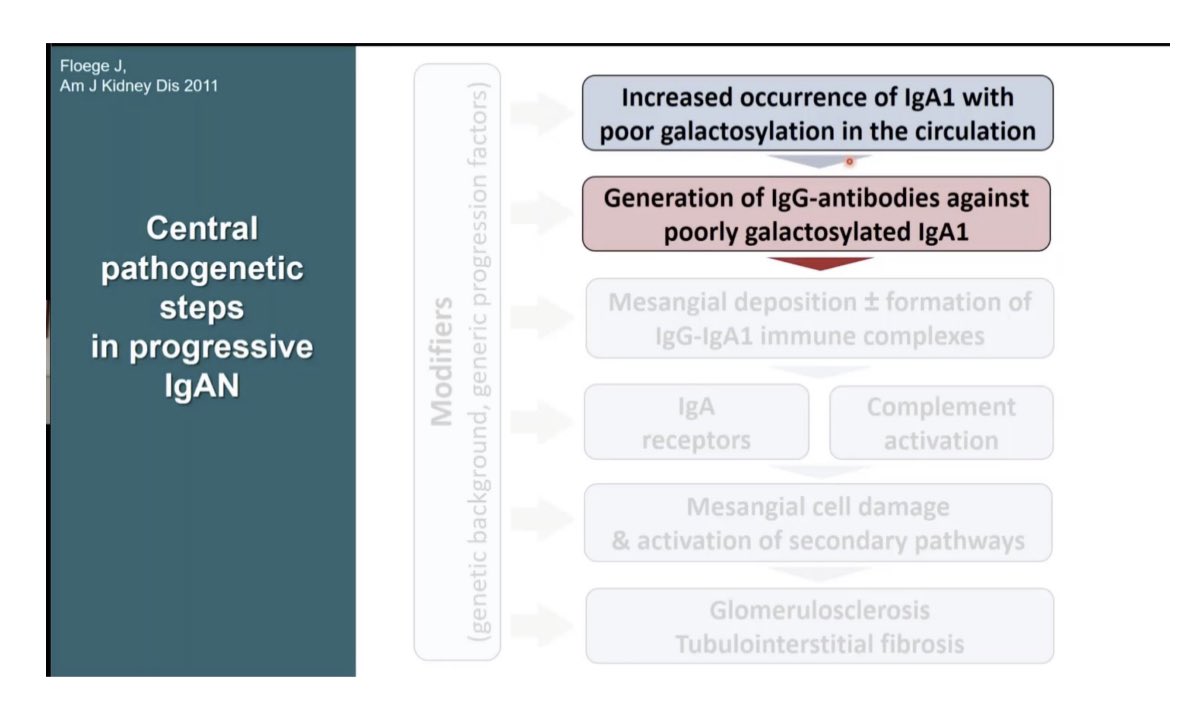
📌 Pathogenesis of IgAN
🔸 First step is increased occurrence of under-galactosylated IgA1 in the circulation
🔸This landmark study showed that the under-galactosylated IgA has a propensity to deposit in the mesangium👇🏽
pubmed.ncbi.nlm.nih.gov/11532091/
10/
🔸 First step is increased occurrence of under-galactosylated IgA1 in the circulation
🔸This landmark study showed that the under-galactosylated IgA has a propensity to deposit in the mesangium👇🏽
pubmed.ncbi.nlm.nih.gov/11532091/
10/


📌 Where is the under-galactosylated IgA produced?
🔸Hypothesis 1: By B-cells in the bone marrow
🔸Hypothesis 2: By mucosal B-cells that translocate from GI tract to the bone marrow.This suggests that pathogenesis of IgAN involves the Gut-Kidney axis
11/
🔸Hypothesis 1: By B-cells in the bone marrow
🔸Hypothesis 2: By mucosal B-cells that translocate from GI tract to the bone marrow.This suggests that pathogenesis of IgAN involves the Gut-Kidney axis
11/

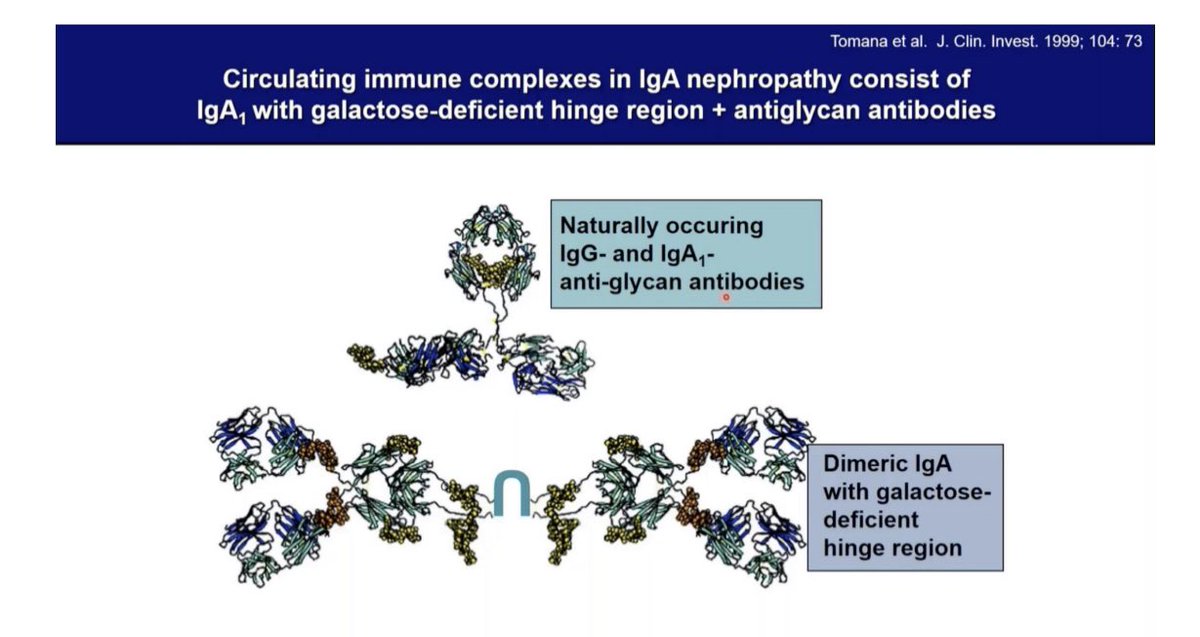
📌 There is evidence that when there is an increase in under-galatactosylated IgA1, it can induce generation of auto-antibodies or the naturally occurring anti-glycan Ab can form immune-complexes which have propensity to deposit in the mesangium👇🏽
12/
12/
📌 The higher the level of these auto-antibodies targeting the under-galactosylated IgA1 -> the higher the risk for progressive kidney disease👇🏽
13/
13/

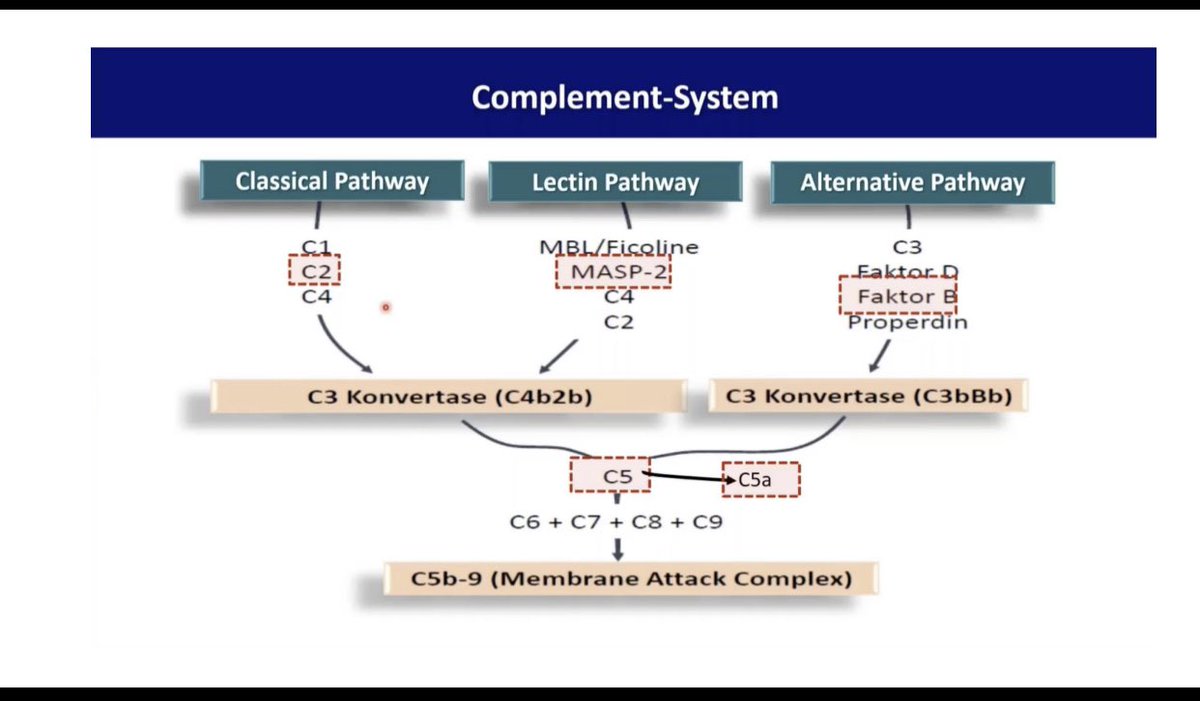
📌 Mesangial deposition and immune complex formation (IgG-IgA1) can lead to complement activation
🔸This is the reason that all pathways of the complement system are being targeted in the on-going IgAN clinical trials👇🏽
14/
🔸This is the reason that all pathways of the complement system are being targeted in the on-going IgAN clinical trials👇🏽
14/

📌 In IgAN, presence of tubulointerstitial fibrosis on kidney biopsy correlates with loss of GFR.
🔸 It remains to be seen if anti-fibrotic therapy would improve outcomes in such cases or not
15/
🔸 It remains to be seen if anti-fibrotic therapy would improve outcomes in such cases or not
15/


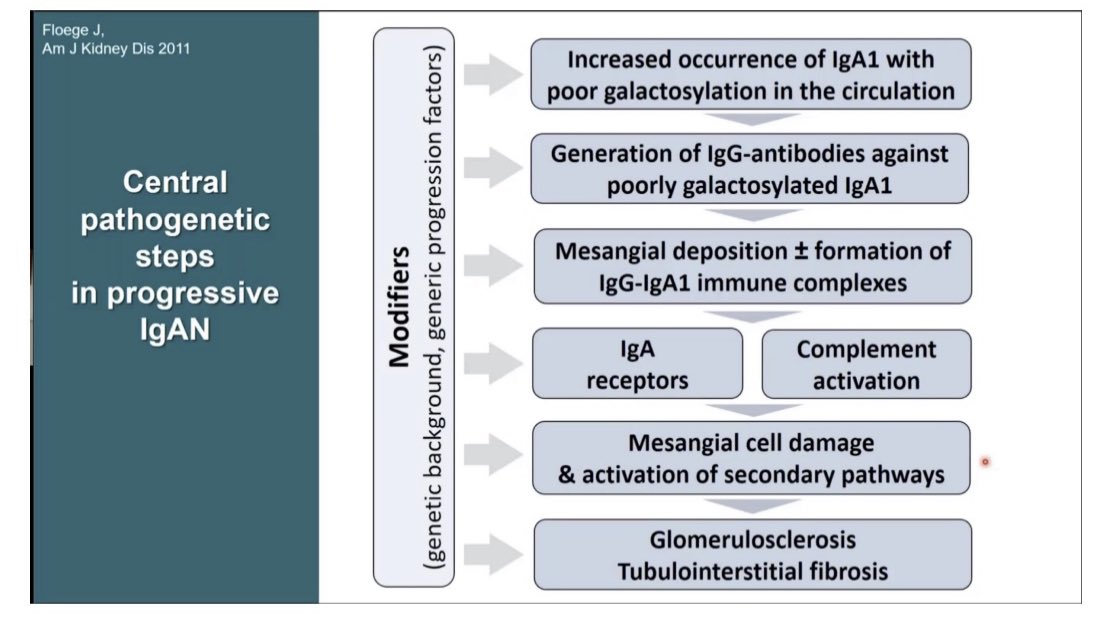
📌 Then there are ‘modifiers’ that can predict if IgAN would be progressive or not. These modifiers can be:
🔸 Genetic factors
🔸 Other generic risk factors such as obesity, HTN, smoking, obesity
16/
🔸 Genetic factors
🔸 Other generic risk factors such as obesity, HTN, smoking, obesity
16/
📌Likelihood of disease progression in benign IgAN: microhematuria, minimal proteinuria, eGFR >60👇🏽
🔸After 20-25 yrs
30% remission
50% proteinuria, preserved GFR
20% progressive CKD
Hard to tell which pts. would develop CKD so follow these pts. closely
17/
🔸After 20-25 yrs
30% remission
50% proteinuria, preserved GFR
20% progressive CKD
Hard to tell which pts. would develop CKD so follow these pts. closely
17/

📌 Supportive therapy in IgAN
🔸BP control
🔸ACEi or ARBs
🔸Lifestyle modifications
📌 Even modest BP lowering can significantly improve outcomes in IgAN👇🏽
18/
🔸BP control
🔸ACEi or ARBs
🔸Lifestyle modifications
📌 Even modest BP lowering can significantly improve outcomes in IgAN👇🏽
18/




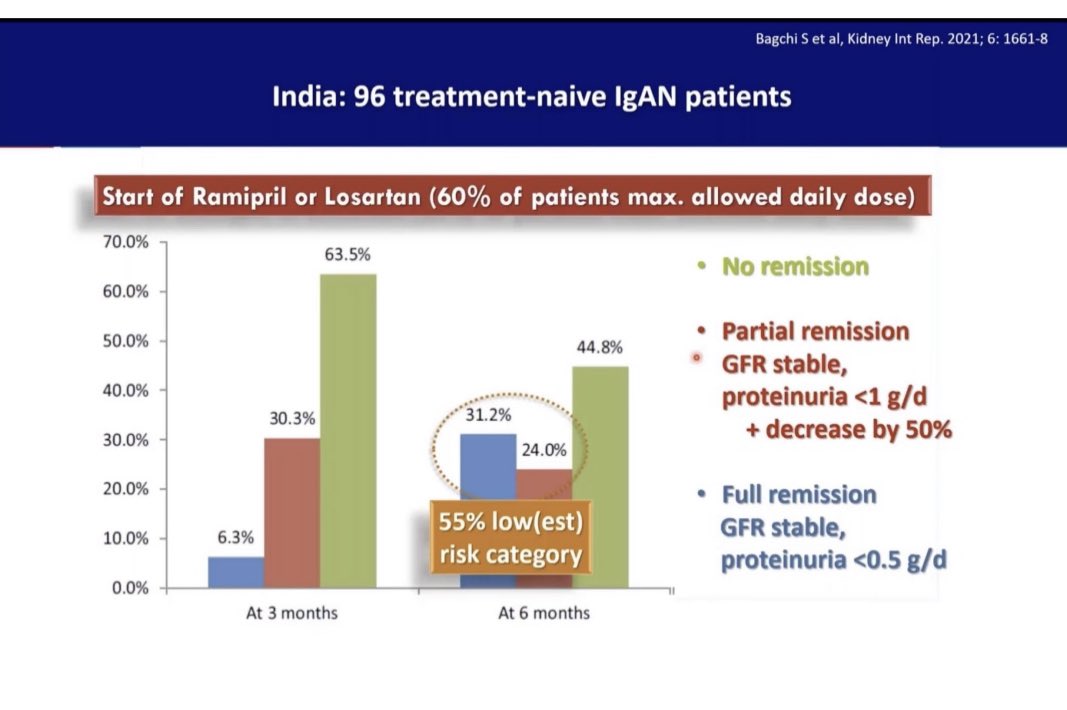
📌 In IgAN the onset of remission following RAAS blocker initiation can take up to 6-months. This study showed that rate of remission at 3-months was 37% and at 6-months it rose to 55%👇🏽
🔸This information is relevant when designing IgAN clinical trials
19/
🔸This information is relevant when designing IgAN clinical trials
19/
📌Assessing prognosis in IgAN
🔸This risk prediction tool can be used
🔸Limitations: based on retrospective data, only validated at the time of biopsy & short follow up
qxmd.com/calculate/calc…
🔸 An updated risk prediction tool will be published soon👇🏽
20/
🔸This risk prediction tool can be used
🔸Limitations: based on retrospective data, only validated at the time of biopsy & short follow up
qxmd.com/calculate/calc…
🔸 An updated risk prediction tool will be published soon👇🏽
20/


📌 Presence of crescents in IgAN is quite common
In a large series of >3000 IgAN patients
🔸<10% crescents were seen in 20-25% pts.
🔸>40% crescents were rarely seen. These pts. can have rapidly progressive disease & require aggressive Rx
21/
In a large series of >3000 IgAN patients
🔸<10% crescents were seen in 20-25% pts.
🔸>40% crescents were rarely seen. These pts. can have rapidly progressive disease & require aggressive Rx
21/


📌 Summary of IgAN pathogenesis:
🔸⬆️ Presence of
under-galactosylated IgA1 in the circulation
🔸Generation of antibodies against under-galactosylated IgA1
🔸Mesangial deposits +/- immune-complex formation
🔸Complement activation
🔸Tissue injury
End/
🔸⬆️ Presence of
under-galactosylated IgA1 in the circulation
🔸Generation of antibodies against under-galactosylated IgA1
🔸Mesangial deposits +/- immune-complex formation
🔸Complement activation
🔸Tissue injury
End/
• • •
Missing some Tweet in this thread? You can try to
force a refresh