
Do transgender persons show sex atypical brains?
Many people suggest that trans people have brains more inline with their desired gender, and this causes feelings of gender incongruence.
However, if we take a closer look, we see some important underlying issues.
Many people suggest that trans people have brains more inline with their desired gender, and this causes feelings of gender incongruence.
However, if we take a closer look, we see some important underlying issues.
In a famous study, the authors compared prepubertal and adolescent children, then suggest sex atypical cerebral differentiation occurs within these individuals.
pubmed.ncbi.nlm.nih.gov/28972892/
pubmed.ncbi.nlm.nih.gov/28972892/
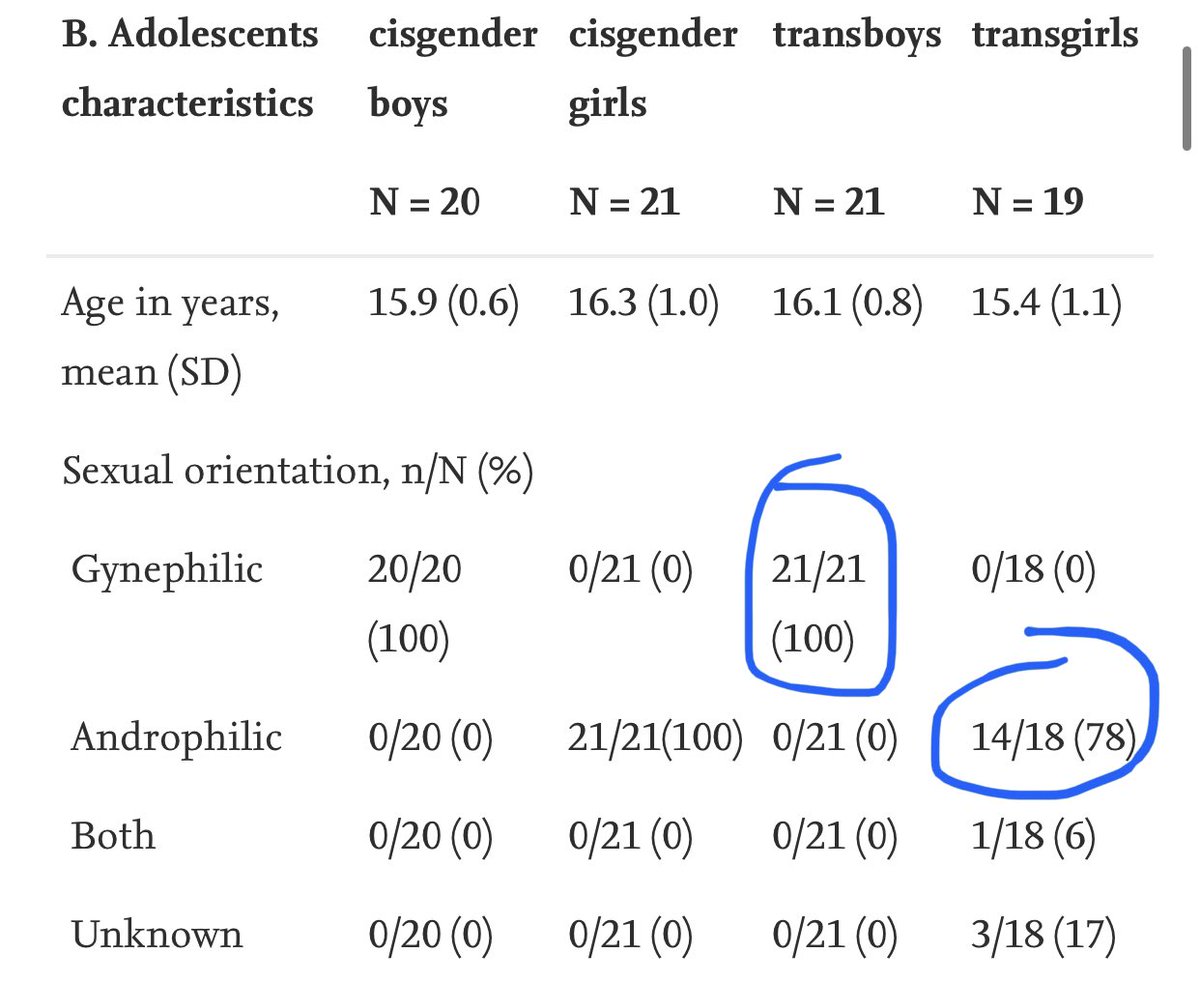
The authors found sex atypical differences in the adolescent cohort (when the majority of the cohort is homosexual)
Homosexuality = 23% of trans boys + 44% of trans girls (prepubertal children; left)
Homosexuality = 100% of trans boys + 78% of trans girls (adolescent; right)
Homosexuality = 23% of trans boys + 44% of trans girls (prepubertal children; left)
Homosexuality = 100% of trans boys + 78% of trans girls (adolescent; right)

The only non-sex typical finding which was specific to gender dysphoria (GD) was in visual network-1 (VN-1; via fMRI)
It was suggested that alterations in this network may disrupt body perception in GD individuals.
It was suggested that alterations in this network may disrupt body perception in GD individuals.
In another study by some of the same authors, they tested whether transgender people (with GD) would have sex atypical hypothalamic activation to androstenedione (a steroid hormone in human sweat that causes sex-specific olfactory responses).
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
But similar to the previous study, sexual orientation was not accounted for.

Why is this important?
Well, the same sex atypical hypothalamic response is observed in homosexual men:
pubmed.ncbi.nlm.nih.gov/15883379/
Well, the same sex atypical hypothalamic response is observed in homosexual men:
pubmed.ncbi.nlm.nih.gov/15883379/
It’s becoming increasingly clear that the only people with any sort of sex atypical cerebral differentiation occurs in homosexual individuals (on average).
This is further supported by functional connectivity studies sex atypical amygdala co-variance
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
You can see this here:
Notice the high similarity in amygdala activity (at rest) between heterosexual females and homosexual males (and vice versa)
Notice the high similarity in amygdala activity (at rest) between heterosexual females and homosexual males (and vice versa)

Interestingly, in an effort to bring all of this together, Savic et al., 2011 examined the brains of heterosexual transgender people in order to control for sexual orientation.
pubmed.ncbi.nlm.nih.gov/21467211/
pubmed.ncbi.nlm.nih.gov/21467211/
The authors found sexual dimorphism in various gray matter parameters in control male and females. However, these findings were NOT found in the heterosexual transgender population.

So rather than sex atypical brain structure/function, what is specific to GD itself?
It’s been shown that individuals with GD show weaker structural & functional connectivity within the default mode network (DMN) of the brain, which is vital for body perception/image and self referential processing
nature.com/articles/s4159…
nature.com/articles/s4159…
Findings which have been replicated here:
pubmed.ncbi.nlm.nih.gov/32057995/
pubmed.ncbi.nlm.nih.gov/32057995/
The DMN consists of cerebral midline structures, including the medial prefrontal cortex (mPFC) and the posterior cingulate cortex (PCC)

Interestingly, it’s been shown that trans individuals (with GD) show a stronger activation pattern within these DMN structures when viewing pictures of their body morphed to the opposite sex
pubmed.ncbi.nlm.nih.gov/31813993/
pubmed.ncbi.nlm.nih.gov/31813993/
You can see the results here:

It’s important to note that correlation is NOT causation. Just because we observe a different pattern in GD subjects compared to neuro-typical controls, doesn’t not suggest it’s innate (born with) or a product of post natal experience. We simply don’t know.
Also, transgender people tend to have lots of co-morbidities from depression, anxiety, anorexia, autism, and a homosexual orientation. All of this needs to be considered when looking at neuroscience studies on this population.
For an overview on molecular hypothalamic differences in relation to homosexuality and gender dysphoria, see thread here:
https://twitter.com/NeuroSGS/status/1550509252921491457
• • •
Missing some Tweet in this thread? You can try to
force a refresh











