One of the difficult aspects of #hemepath training is time management in a high-paced/demanding environment & the ability to multitask effectively while learning a difficult discipline. Every yr I offer our fellows helpful tips I’ve learned so far 🧵👇🏻More tips welcome,pls add 1/ 

Get rid of paper…
Don’t do anything twice
Take ownership of your cases… they are just as much yours as they are your faculty’s
Don’t do anything twice
Take ownership of your cases… they are just as much yours as they are your faculty’s

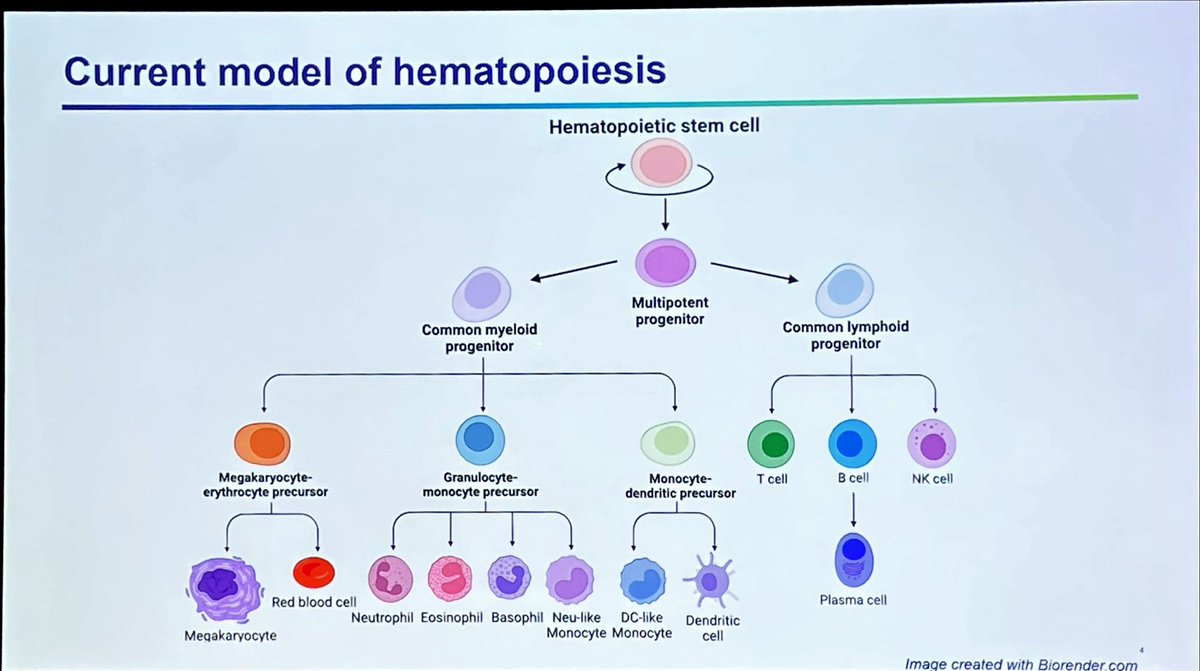
Use online learning tools… like great #hemepath modules here on @PathElective @KMirza @cullen_lilley

Bookmark your frequently visited websites… saves you a lot of time over the year… here are some of mine! Shoutout to @hematogones for his awesome BM diff calculator

Use social media… it will accelerate your learning, networking opportunities and will expand your professional circle

Your time is your most valuable commodity! I realize you don’t make a lot of money as a trainee but invest in yourself… use your time wisely… it’s ok to accumulate some debt!

Aim for perfection…. Your definition of perfection will evolve with time… don’t shortchange yourself!! This is your opportunity to learn!!

And finally…. Appreciate the opportunity you have as a trainee… this is your only time to make mistakes that are mostly inconsequential….the goal is to learn from your mistakes!! Give yourself the time and freedom to learn and enjoy yourself…. Happy learning all!!!

• • •
Missing some Tweet in this thread? You can try to
force a refresh